 Subscribe To This Site Subscribe To This Site |
Home > Rn Test Kits & Monitors > Radon Gas Guide What Is Radon Gas? |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



You too likely have a higher risk of Lung Cancer as a result of Radon Gas entering your home from below. This extensive guide will answer all your questions about testing for and reducing your exposure to this hazard infiltrating into your home from the earth below.
Radon Map Showing Gas Levels Are Often Elevated Where Granite is Common
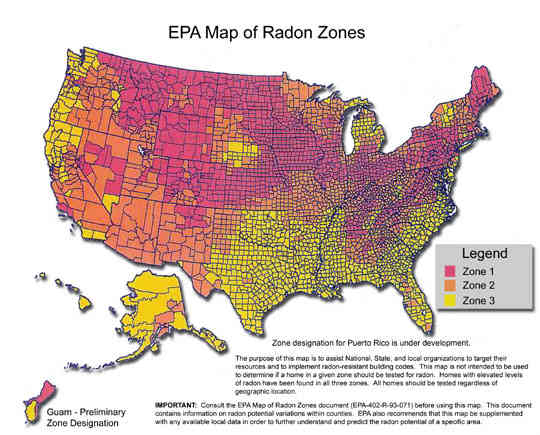 |
As you can see from the above EPA Radon Zone Map, the areas of the U.S. with higher potential for elevated Radon Gas levels are also those areas where Granite stone and fractured rocky earth is typical. |
FACT: Radon Gas is a cancer causing redioactive gas emmitted from the Earth's crust. Radon is the second leading cause of Lung Cancer in the U.S. and amounts to health care costs in excess of $2 Billion annually. Most damage to the lungs results from direct Radon inhalation as well as from it's decay products like Bismuth, Lead, and Polonium which stick to inhalable dust particles in the air.
This extensive guide to Radon Gas includes FAQs, public health information, state resources, information about Radon testing, toxicological information, Radon mitigation information, Radon MSDS, and many more resources about this second leading cause of lung cancer.
Radon Gas: A Stealthy Killer
At the EPA's action guideline Radon level of 4pCi/l the risk of death is 1 in 100 which is 1,000 times the risk of death of any other EPA carcinogen! The only way to know the Radon levels in your home is through Radon testing. It is colorless, odorless, and inhalation of it causes no emmediately identifiable symptoms. So have your home tested for Radon gas ASAP - it is a very stealthy killer.
Indoor Radon levels can fluctuate vastly from one home to the next depending on many factors including how a home is constructed or nearby geological features such as cracks in rocks or soil composition. So even if your neighbor's home tests low for Radon gas, your home could still test high.
According to the EPA, 1 in 15 homes has elevated levels of Radon gas. But there really is no safe level. I highly recommend you test your home to know if source control via a Radon Reduction System is needed.
Cigarette Smoke + Radon Exposure
Cigarette Smokers who live in a home with elevated levels of Radon are at extreme risk of lung cancer because Radon decay products such as lead particles have been shown to attach to already highly toxic cigarette smoke particles on which they may hitch a ride and be inhaled deep into the lungs.
Plus cigarette smoke itself has been proven to contain radioactive Polonium and other metal isotopes which originally attached to dust particles which then often collect on the resinous tobacco leaves while still in the fields.
The smoke and radioactive gas decay energy and particles are also thought to have a synergistic effect for causing lung cancer. That means the total damage to your lungs from both air pollutants is much more than the sum of the damage that each would cause separately.
Others in the household who are exposed to Secondhand smoke and elevated Radon, may also experience much elevated Lung Cancer risk, especially children who have faster dividing cells and less body mass.
Chart Showing Radioactive Decay of Uranium-238 into Radon, Daughter Nuclides, and Alpha / Beta Radiation
 |
As radioactive decay of Uranium occurs in Earth's crust, Radon Gas is created which often infiltrates into homes from lower levels. When the Radon gas itself decays, it produces a chain of variously unstable decay daughter elements along with alpha and beta radiation releases at each step. When you inhale dust carrying these elements, the chain reaction into toxic metals and ionizing radiation can damage your lung tissues and cellular DNA directly, resulting in a much elevated risk of Lung Cancer. This scenario may be multiplied exponentially for cigarette smokers also exposed to elevated Radon levels indoors. |
Home Air Purifiers for Radon Control?Unfortunately Home air purifiers are not considered an effective method of radon removal nor are they effective at controlling exposure to the radioactive gas.
The only air purification devices that might absorb the gas would involve special activated carbon filters, which a few air purifiers contain. However, activated carbon not only becomes saturated relatively quickly and must be replaced, it also has been shown to not bind Radon permanantly.
Likewise, the gas could not be captured practically given that it is difficult to clean all the air in a home consistently using home air purifiers. So overall the most successful way to limit exposure to Radon gas is to control it at its point of source which is usually located in the basement or crawlspace of your home.
Methods of Radon mitigation and Radon proof construction techniques exist which will limit or prevent the gas from entering living spaces. Information on various methods of testing and Radon remediation are discussed in detail below.
Best Ways of Testing for Radon Gas
Radon testing to determine if gas levels in a home is elevated is the most important first step any homeowner can take to determine if a Radon repair and removal plan involving such methods as suction, radon fan, venting, or radon seal will be needed.
I have created a page based on my Radon experience which will show you How to Test for Radon Gas Levels in Your Home - Simply, Cheaply, and Accurately.
Public Health Statement for Radon GasCONTENTS: 1.2 How might I be exposed to Radon gas? 1.3 How can Radon gas enter and leave my body? 1.4 How can Radon gas exposure affect my health? 1.5 What levels of Radon exposure have resulted in harmful health effects? 1.6 Is there a medical test to determine whether I have been exposed to Radon? 1.7 What recommendations has the federal government made to protect human health from Radon gas? 1.8 Where can I get more information about Radon gas? Who is at risk from Radon Gas? Respiratory Dose and Units of Measure Table 1. Radon Risk Evaluation Chart if You Smoke Table 2. Radon Risk Evaluation Chart if You Have Never Smoked Radon Toxicity - Physiological Effects Radon Toxicity - Treatment and Management Radon Toxicity - Radon Abatement Radon Toxicity - Standards and Regulations Table 3. Residential Standards and Regulations for Radon Table 4. Occupational Standards and Regulations for Radon Radon Toxicity - Sources of Information Radon Toxicity - Suggested Reading 1.11 Complete Radon MSDS and Toxicological Information for Radon Gas This Statement was prepared to give you information about radon and to emphasize the human health effects that may result from exposure to it. The Environmental Protection Agency (EPA) has identified 1,177 sites on its National Priorities List (NPL). Radon has been found above background levels at five of these sites. However, we do not know how many of the 1,177 NPL sites have been evaluated for radon. As EPA evaluates more sites, the number of sites at which radon is found may change. The information is important for you because radon may cause harmful health effects and because these sites are potential or actual sources of human exposure to radon. When a radioactive chemical is released from a large area such as an industrial plant, or from a container such as a drum or bottle, it enters the environment as a radioactive chemical, This emission, which is also called a release, does not always lead to exposure. You can be exposed to a chemical only when you come into contact with the chemical. You may be exposed to it in the environment by breathing, eating, or drinking substances containing the chemical or from skin contact with it. If you are exposed to a hazardous substance such as radon, several factors will determine whether harmful health effects will occur and what the type and severity of those health effects will be. These factors include the dose (how much), the duration (how long), the route or pathway by which you are exposed (breathing, eating, drinking, or skin contact), the other chemicals to which you are exposed, and your individual characteristics such as age, sex, nutritional status, family traits, life style, and state of health. 1.1 What is radon?Radon is a naturally occurring colorless, odorless, tasteless radioactive gas that is formed from the normal radioactive decay of uranium. Uranium is present in small amounts in most rocks and soil. It slowly breaks down to other products such as radium, which breaks down to radon. Some of the radon moves to the soil surface and enters the air, while some remains below the soil surface arid and enters the groundwater (water that flows and collects underground). Uranium has been around since the earth was formed and has a very long half-life (4.5 billion years), which is the amount of time required for one-half of uranium to break down. Uranium, radium, and thus radon, will continue to exist indefinitely at about the same levels as they do now. Radon gas also undergoes radioactive decay and has a radioactive half-life of about 4 days. This means that one-half of a given amount of radon will be changed or decayed to other products every 4 days. When radon decays, it divides into two parts. One part is called radiation, and the second part is called a daughter. The daughter, like radon, is not stable; and it also divides into radiation and another daughter. Unlike radon gas, the daughters are metal and easily attach to dust and other particles in the air. The dividing of daughters continues until a stable, nonradioactive daughter is formed. During the decay process, alpha, beta, and gamma radiations are released. Alpha particles can travel only a short distance and cannot go through your skin. Beta particles can penetrate your skin, but they cannot go all the way through your body. Gamma radiation, however, can go all the way through your body. Thus there are several types of decay products that result from radon gas decay. Synonyms: Since radon is a gas and radon daughters are often attached to dust, you are exposed to them primarily by breathing them in. They are present in nearly all air. However, background levels of radon in outdoor air are generally quite low, about 0.003 to 2.6 picocuries of radon per liter of air. A picocurie is a very small amount of radioactivity equal to one quintillionth (1/1018) of an ounce of radon. In indoor locations, such as homes, schools, or office buildings, levels of radon and daughters are generally higher than outdoor levels. Indoor radon levels are generally about 1.5 picocuries radon per liter of air. Cracks in the foundation or basement of your home may allow increased amounts of radon to move into your home. You may also be exposed to radon and daughters by drinking water obtained from wells that contain radon. Average levels of radon in groundwater are about 350 picocuries of radon per liter of water. However, most radon in water is rapidly released into the air and can be breathed in. In some areas of the country the amount of uranium and radium in some rock types, such as phosphate or granite, is high. In these areas radon levels in outdoor air or in groundwater will generally be higher. In most cases, radon entering the home through water will be a small source of risk compared with radon entering from the soil. EPA estimates that indoor radon levels will increase by about 1 pCi/L for every 10,000 pCi/L of radon in water. Only about one to two percent of indoor radon in air comes from drinking water.Based on a National Academy of Science report, EPA estimates that radon in drinking water causes about 168 cancer deaths per year: 89 percent from lung cancer caused by breathing released to the indoor air from water and 11 percent from stomach cancer caused by consuming water containing radon. Radon gas can enter the home through well water. It can be released into the air you breathe when water is used for showering and other household uses. Research suggests that swallowing water with high radon levels may pose risks, too, although risks from swallowing water containing radon are believed to be much lower than those from breathing air containing radon. While radon in water is not a problem in homes served by most public water supplies, problems have been found in well water. If you've tested the air in your home and found a radon problem, and your water comes from a well, contact a lab certified to measure radiation in water to have your water tested. Call EPA's Safe Drinking Water Hotline, (800) 426-4791 to get information on locating a certified lab. If you're on a public water supply and are concerned that radon may be entering your home through the water, call your public water supplier. Radon and its radioactive daughters can enter your body when you breathe them in or swallow them. By far, the greater amounts are breathed in. Most of the radon is breathed out again. However, some radon and most of the daughters remain in your lungs and undergo radioactive decay. The radiation released during this process passes into lung tissue and is the cause of lung damage. Some of the radon that you swallow with drinking water passes through the walls of your stomach and intestine. After radon enters your blood stream most (greater than 90%) of the radon goes to the lungs where you breathe most of it out. This occurs very shortly after it is taken in. Any remaining radon undergoes decay. Radon that does not go to the lungs goes to other organs and fat where it may remain and undergo decay. There is very limited information on whether radon gas can penetrate the skin, but some radon may be able to pass through the skin when you bathe in water containing radon. back to top
Long-term exposure to radon and radon daughters in air increases your chances of getting lung cancer. When exposures are high, noncancer diseases of the lungs may occur, such as thickening of certain lung tissues. While noncancer health effects may occur within days or weeks after exposure to radon, it will be several years before cancer effects become apparent. This is known from studies of workers exposed to radon in mines, primarily uranium miners, and from tests on laboratory animals. Although radon is radioactive, it gives off little gamma radiation. Therefore, harmful health effects of radon gas from external exposure (when the chemical does not come into direct contact with your body) are not likely to occur. In addition, it is not known if radon causes health effects other than to the lung. Also, the health effects of exposure to radon in water or from radon in food are not known. back to top
In studies of uranium miners, workers exposed to radon levels of 50 to 150 picocuries of radon per liter of air for about 10 years have shown an increased frequency of lung cancer. Although there is some uncertainty as to how much exposure to radon increases your chances of getting lung cancer, the greater your exposure to radon, the greater your chance of developing lung cancer. Even small exposures may increase your risk of developing lung cancer, especially if you smoke cigarettes. There is no information on the effects of radon if you drink water or eat food containing radon. back to top
Radon in human tissues is not detectable by routine medical testing. However, several of its decay products can be detected in urine and in lung and bone tissue. These tests, however, are not generally available to the public and are of limited value since they cannot be used to accurately determine how much radon you were exposed to, nor can they be used to predict whether you will develop harmful health effects. back to top
The EPA has set an effective dose equivalent for the public of 10 millirems per year (10 mrem/yr) for radon emissions from underground uranium mines. The EPA has also set a standard of 20 picocuries per square centimeter per second (20 pCi/m²/sec) for emissions of radon-222 (a radon daughter) to the air from uranium mill tailings in non-operational piles. The federal recommendations have been updated as of July 1999. back to top
If you have any more questions or concerns, please contact your community or state health or environmental quality department or: Agency for Toxic Substances and Disease Registry Information line and technical assistance: Phone: 888-422-8737 ATSDR can also tell you the location of occupational and environmental health clinics. These clinics specialize in recognizing, evaluating, and treating illnesses resulting from exposure to hazardous substances. To order toxicological profiles, contact: National Technical Information Service National Radon Fix-It Program - Lowering Radon Levels: Help for Consumers With Radon in Home The National Safety Council, a non-profit organization, operates the Radon Fix-It Program free of charge. The Radon Fix-It Program provides guidance to consumers with elevated radon levels (4 pCi/L or higher) to take the necessary steps towards radon testing and fixing their homes, also known as radon mitigation. The Radon Fix It Program operators provide referrals to technical experts in your state government, information on reducing elevated radon levels, information on choosing a radon test kit or a testing company, information about radon monitoring, information about a particular radon mitigation system, and information about testing in connection with a real estate transaction. They also provide lists of contractors certified by the National Environmental Health Association and/or the National Radon Safety Board who are qualified to offer radon abatement advice, perform radon mitigation or radon gas test, and radon detection. They may also be able to suggest a radon kit, digital radon detector, useful tips for radon gas testing, instructions for radon remediation, home radon repair, methods of radon gas protection, or methods of radon removal. The toll-free Radon Fix It Program is for people whose radon test results are 4 pCi/L or higher. People with elevated radon levels should call (800) 644-6999 for further information about radon mitigation systems to remove radon in a home which may involve radon repair methods such as the radon seal techniques, radon fan, radon suction fan, and other types of cost effective radon removal from new and existing homes. Useful Links to More Radon Information:
Agency for Toxic Substances and Disease Registry (ATSDR). 1990. Toxicological profile for radon. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. back to topContents:Who is at risk from Radon Gas? Respiratory Dose and Units of Measure Table 1. Radon Risk Evaluation Chart if You Smoke Table 2. Radon Risk Evaluation Chart if You Have Never Smoked Radon Toxicity - Physiological Effects Radon Toxicity - Treatment and Management Radon Toxicity - Radon Abatement Radon Toxicity - Standards and Regulations Table 3. Residential Standards and Regulations for Radon Table 4. Occupational Standards and Regulations for Radon Radon Toxicity - Sources of Information Radon Toxicity - Suggested Reading Radon, like Asbestos, is a natural yet potentially harmful product of our planet. Hazardous Radon gas results from the decay of Uranium within Earth's crust and mantle. This radioactive decay of Uranium to Radon is a primary source of the heat which helps to turn solid rock into molten magma within our little blue marble. We are in essence living on a massive thermo-nuclear reactor thanks to the formation of Radon! It's no wonder Radon has been detected in many homes throughout all 50 U.S. states. In fact, no matter where on this world you stand, the process of Radon formation and subsequent surface emmission, is most likely occuring right below your feet!...But don't panic just yet! Instead take a deep breath and marvel at the natural environment in which we all live. "The formation of Radon has been a "neccessary evil" for the metamorphosis to the planet as we know it today."The atmosphere and weather, the plentiful oceans rivers and lakes, the varied landscapes, and all creatures great and small pretty much all owe their existance to the process of Radon formation. Really! From the Earth's internal thermal convection and resultant plate techtonics which sculpts the landmasses, to the first rain drops which fell on the cooling primordial Earth, the formation of Radon has been a "neccessary evil" for the metamorphosis to the planet as we know it today. "But as Radon gaveth life, so may it taketh away!"Radon is second only to smoking as a cause of lung cancer deaths in the U.S. It is estimated that more than 20,000 people die each year from Radon related lung cancer. However, for those who also smoke or were exposed to Environmental Tobacco Smoke (ETS or second-hand smoke), radon exposure will result in a dramaticly higher rate of lung cancer. Radon concentration and duration of exposure are also two primary factors used in Radon risk assessments. Radon has quickly advanced up the list of harmful indoor air pollutants because as our dwellings become more and more air tight for energy efficiency sake, the gas is trapped inside and can increase in concentration with time. Worse yet, you can not see, taste, or smell Radon. Consequently, there are no obvious clues as to its presence despite it being a common airborn contaminant in the air of homes, offices, schools, and many other buildings. However, Radon breaks down into harmful radiation and paricles which can be detected in homes using a Radon test kit. The EPA's guideline value for suggested Radon remediation is 4 pCi/L Radon, though there is no safe level of exposure concerning Radon or it's toxic by-products. The USEPA's guideline value of 4 pCi/L is the lowest concentration of Radon that could be achieved in the late 1970s when highly contaminated houses built on Uranium waste were tested after using control technologies that were 99% effective. It is now the standard level used to determine if there is a Radon safety issue needing remediation. Approximately 1 out of every 3 Midwest homes contains Radon levels in excess of 4 pCi/L when a short term Radon test kit was used. These higher incidents seem to correlate with highly granitic soils, but not in all cases. A 3 to 6 month average Radon level is needed to get an accurate diagnosis of whether Radon remediation is needed because the EPA's guideline value of 4 pCi/L Radon is based on exposure of Radon over a one year period. "Radon is also typically twice as concentrated in the basement compared to upstairs living areas"Radon gas and its by-products escape from the soil and tend to accumulate in basement or crawlspace air. Therefore, houses with basements tend to have higher concentrations of Radon compared to non-basement houses. Radon is also typically twice as concentrated in the basement compared to upstairs living areas so unless one lives in a basement area exposure to Radon is often much less than test results may indicate if Radon testing was performed in the basement. Radon testing should be performed on all levels of the dwelling below the 3rd floor. "Most problems with radon in the home can be fixed for between $800 and $2500."If a short term Radon test kit indicates Radon remediation may be required several methods may reduce Radon in a home. Some Radon remediation systems can cost effectively reduce Radon levels up to 99%. Most problems with radon in the home can be fixed for between $800 and $2500. One example, the soil suction radon reduction system involves a vent pipe system and Radon fan to evacuate contaminated air from crawlspaces or basement areas where Radon is typically in the highest concentrations. The installation of this Radon mitigation system involves no major changes to the home. Radon fans are especially designed for radon mitigation by exhausting air outward. These Radon fans will not typically corrode as rapidly as a regular fan. Because of this, Radon fans can often be used for removing moist air from basements and crawlspaces as well as for radon removal. Another method of Radon gas protection involves the use of air tight Radon seals where the Radon escapes from the Earth below a home. These Radon seals may be used in conjunction with Radon fans for an effective Radon removal system. Regular Radon monitoring should be used to verify the effectiveness of any Radon mitigation system. Radon ToxicityWho is at Risk
History of RadonAs early as the 16th century, Paracelsus and Agricola described a wasting disease of miners. In 1879, this condition was identified as lung cancer by Herting and Hesse in their investigation of miners from Schneeberg, Germany. Radon itself was discovered some 20 years later by Rutherford. Subsequently, an increase in the incidence of lung cancer among miners was linked to radon daughter exposure in mines. Underground uranium mines found throughout the world, including the western United States and Canada, pose the greatest risk because of their high concentration of radon daughters in combination with silica dust, diesel fumes, and, typically, cigarette smoke. Iron ore, potash, tin, fluorspar, gold, zinc, and lead mines also have significant levels of radon, often because of radium in the surrounding rock. In the past, it was not uncommon to use the tailings from these mines as fill on which to build homes, schools, and other structures. Indoor radon daughters have been widely recognized as a potential problem in Europe and the Scandinavian countries since the 1970s. Public awareness in the United States was heightened in December 1984, when "Worker A" at the Limerick nuclear plant in Pennsylvania began setting off radiation alarms when he entered the plant. The cause was traced to levels of excessive radon daughters in his home-500 times the level at which the U.S. Environmental Protection Agency (EPA) recommends remediation (i.e., 4 picocuries per liter [pCi/L]). Radon daughters attach to dust particles in the air that are attracted to items such as clothing, especially when the air is cold and dry. In 1987, the federal government allotted $10 million to the states to determine the extent of radon contamination in homes and schools, and subsequently amended the Toxic Substances Control Act to assist the states "in responding to the threat to human health posed by exposure to radon." In 1988, EPA and the Office of the Surgeon General jointly recommended that all US homes below the third floor be tested for radon. In 1990, Congress appropriated $8.7 million for grants to states to develop and enhance programs to reduce radon risk in homes and schools. It has become standard practice in some states to measure radon levels in homes at the time of real estate transactions. Radon testing is required for all government buildings.
The amount of radon emanating from the earth and concentrating inside homes varies considerably by region and locality, and is greatly affected by the residential structure as well as soil and atmospheric conditions. Nearly every state in the United States has dwellings with measured radon levels above acceptable limits. EPA estimates that 6% of American homes (approximately 6 million) have concentrations of radon above 4 pCi/L. In Clinton, New Jersey, near a geologic formation (the Reading Prong) that is high in radium, all 105 homes tested were above the recommended guidelines; the levels in 40 homes exceeded 200 pCi/L. In the "Worker A" home, levels of 2,700 pCi/L were found in the basement. Areas of the country that are likely to have homes with elevated radon levels are those with significant deposits of granite, uranium, shale, and phosphate, which are all high in radium content and, therefore, potential sources of radon gas. Some homes in these areas, however, might not have elevated levels of radon. Because of the many determinants of indoor radon levels, local geology alone is an inadequate predictor of risk. The only way to determine indoor radon concentration is by testing. A home 100 feet away from the "Worker A" home did not have measured radon concentrations that required remediation, yet both houses were on the same geologic formation. Other factors that predispose homes to elevated levels of radon include soil porosity, foundation type, location, building materials used, entry points for soil gas, building ventilation rates, and source of water supply. Further research is being conducted on ways to predict which homes are most likely to have significant levels of radon.
Several studies have shown that smokers exposed to radon are at greater risk for lung cancer than are similarly exposed nonsmokers. It is generally believed that exposure to radon and cigarette smoking are synergistic; that is, that the combined effect exceeds the sum of their independent effects. The risk of lung cancer from radon exposure is estimated to be 10 times greater for persons who smoke cigarettes in comparison with those who have never smoked. According to the National Academy of Sciences Committee on the Biological Effects of Ionizing Radiation (BEIR VI), a breakdown of the contribution of smoking and radon exposure to lung cancer deaths in the United States illustrates that of every 100 persons who died of lung cancer, approximately 93 were current or former smokers, whereas 7 had never smoked. Data on the effects of radiation in children are limited, and even less is known about the effects of radon exposure in this age group. Cancer development in Japanese atomic bomb survivors suggests an increased susceptibility to radiation in children compared to that in adults. Children also have different lung architecture, resulting in a somewhat larger dose of radiation to the respiratory tract, and children have longer latency periods in which to develop cancer. However, no conclusive data exist on whether children are at greater risk than adults from radon.
Radon Toxicity | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radon Level | If 1,000 People Who Smoked Were Exposed to This Level Over a Lifetime... | The Risk of Cancer From Radon Exposure Compares to... | What To Do: STOP SMOKING and... |
|---|---|---|---|
| 20 pCi/L | About 250 men or 143 women could die of lung cancer | > 100 times the risk of drowning | Consider fixing between 2 and 4 pCi/L |
| 8 pCi/L | About 132 men or 66 women could die of lung cancer | > 100 times the risk of dyingin a home fire | Consider fixing between 2 and 4 pCi/L |
| 4 pCi/L | About 66 men or 33 women could die of lung cancer | > 100 times the risk of dying in an airplane crash | Consider fixing between 2 and 4 pCi/L |
| 2 pCi/L | About 33 men or 16 women could die of lung cancer | > 2 times the risk of dyingin a car crash | Consider fixing between2 and 4 pCi/L |
| 1.0 pCi/L | About 16 men or 8 women could die of lung cancer | (Average indoor radon level) | (Reducing radon levels below 2 pCi/L is difficult) |
| 0.4 pCi/L | About 8 men or 4 women could die of lung cancer | (Average outdoor radon level) | |
| *pCi/L: picocuries per liter. If you are a former smoker, your risk might be lower. | |||
Table 2. Radon Risk Evaluation Chart if You Have Never Smoked
| Radon Level | If 1,000 People Who Never Smoked Were Exposed to This Level Over a Lifetime... | The Risk of Cancer From Radon Exposure Compares to... | What To Do: |
|---|---|---|---|
| 20 pCi/L | About 33 men or 20 women could die of lung cancer | > 2 times the risk of being killed in a violent crime | Consider fixing between2 and 4 pCi/L |
| 8 pCi/L | About 13 men or 8 women could die of lung cancer | Consider fixing between 2 and 4 pCi/L | |
| 4 pCi/L | About 6.4 men or 4 women could die of lung cancer | > 10 times the risk of dying in an airplane | Consider fixing between 2 and 4 pCi/L |
| 1.0 pCi/L | About 1.6 men or 1 woman could die of lung cancer | The risk of dying in a home fire (Average indoor radon level) | (Reducing radon levels below 2 pCi/L is difficult) |
| 0.4 pCi/L | Less than 1 person could die of lung cancer | (Average outdoor radon level) | |
| *pCi/L: picocuries per liter. If you are a former smoker, your risk might be higher. | |||
Radon Toxicity
Physiologic Effects
- The primary adverse health effect of exposure to radon daughters is lung cancer.
Radon exposure causes no acute or subacute health effects, no irritating effects, and has no warning signs at levels normally encountered in the environment. The only established human health effect associated with residential radon exposure is lung cancer. Epidemiologic studies of miner cohorts have reported increased frequencies of chronic, nonmalignant lung diseases such as emphysema, pulmonary fibrosis, and chronic interstitial pneumonia, all of which increased with increasing cumulative exposure to radiation and with cigarette smoking.
- The synergistic mechanism(s) of cigarette smoking and radon exposure are not known, although the adverse health effects of the combination are clear.
Epidemiologic studies and a recent study of groundwater radon and cancer mortality have found no association with extrapulmonary cancers, such as leukemias and gastrointestinal cancers. This is expected on the basis of studies of the radium-dial painter population. Evidence is also lacking that environmental radon exposure is causally associated with adverse reproductive effects.
- Radon progeny can be inhaled either as free particles or attached to dust. Attached progeny preferentially deposit in the bronchi, the site of most lung cancers.
Because of their charged state and solid nature, radon progeny rapidly attach to most available surfaces, including walls, floors, clothing (as in the case of "Worker A"), and airborne particulates. Radon progeny can be inhaled, therefore, either as free, unattached particles or attached to airborne dust. Smaller dust particles can deposit radon progeny deep in the lungs. Because they are ionized, the progeny tend to attach to the respiratory epithelium. Through mucociliary action, the progeny are eventually cleared from the respiratory tract, but because of their short half-life, they can release alpha particles before being removed. The total amount of energy deposited by the progeny is several hundred times that produced in the initial decay of radon. When these emissions occur within the lungs, the genetic material of cells lining the airways can be damaged, resulting in lung cancer.
The risk of lung cancer due to radon exposure is thought to be second only to that of smoking. The synergism between cigarette smoking and radon places the large population of current and former smokers at particularly high risk for lung cancer. Although the net consequence of cigarette smoking and exposure to radon decay products has been clearly demonstrated in smokers, the mechanism of interaction is still unclear.
Most of the lung cancers associated with radon are bronchogenic, with all histologic types represented. However, small-cell carcinoma occurs at a higher frequency among both smoking and nonsmoking populations of underground miners in the initial years after exposure, compared to the pattern of histologic types in the general population. Other types of lung cancers seen in radon-exposed miners are squamous cell carcinoma, adenocarcinoma, and large-cell carcinoma.
Treatment and Management
- Generally, the most effective methods to reduce the risk of lung cancer are smoking cessation and radon mitigation.
No effective communitywide screening methods are available for medical prevention or early diagnosis and treatment of lung cancer (radon-induced or otherwise). Routine chest radiographs and sputum cytology are ineffective for screening lung cancer associated with cigarette smoking and would presumably be ineffective for screening lung cancer associated with radon as well. The most effective methods of prevention are reduction of radon exposure and modification of other simultaneous risk factors for lung cancer, such as smoking. The only long-term solution for reducing the risk of lung cancer is smoking cessation, coupled with detection and mitigation of high radon levels.
- The potential risk of cancer due to radon poisoning is often underestimated by the public; this bias might discourage assessment and abatement measures in the home.
Several studies have noted optimistic biases in the public's assessment of the risk due to radon. A New Jersey study found that this bias might discourage testing and subsequent implementation of control measures. In Maine, homeowners were found to greatly underestimate the potential risk, and abatement behavior was not significantly related to potential risk.
Primary care physicians and public health professionals should promote public awareness so that the radon safety problem is seen in the proper perspective, leading to appropriate mitigation action when indicated. Physicians and public health officials should therefore test their own homes and offices to relate their experience to others and to provide guidance on how to carry out the testing.
Radon Toxicity
Radon Detection
Radon levels cannot be accurately predicted solely on the basis of factors such as location, geology, building materials, and ventilation. Measurement is the key to identifying the problem. Radon detection kits are available in most hardware stores.
Short-term testing (lasting a few days to several months) is the quickest way to determine if a potential problem exists. Charcoal canisters, liquid scintillation detectors, electret ion detectors, alpha-track detectors, and continuous monitors are the most common short-term testing devices. Short-term testing should be conducted in the lowest inhabited area of the home, with the doors and windows shut.
Long-term testing (lasting up to 1 year) will give a better reading of a home's year-round average radon level than will a short-term test. Alpha-track detectors and electret ion detectors are the most common long-term testing devices. Exposed devices are sent via mail to a certified laboratory for analysis. These devices measure radon gas levels, rather than radon progeny; thus, the units reported are in picocuries of radon per liter of air.
The charcoal canister is a small can containing charcoal and a filter to keep out radon progeny. It is inexpensive ($10 to $25) and is generally used for short-term testing (3 to 7 days). The alpha-track device contains a small piece of plastic in a filtered container. As the radon gas that has entered the container decays, the alpha particles form etch tracks. These tracks can be counted using a special technique. The cost of the alpha-track device is roughly twice that of the charcoal canister, and it can be used to measure cumulative exposure over a longer period (i.e., several weeks to a year).
Congress has mandated that each state set up an office to deal with requests for radon assistance. Many states provide radon detection kits such as the charcoal canister free of charge as a public service. A list of state radon contacts can be found in the Sources of Information section.
Radon Abatement
- The cost of remediation to reduce radon levels in the average home is about $1,200.
- Available procedures to lower indoor radon levels are, dollar for dollar, very effective in saving lives.
How cost-effective is radon mitigation compared to other investments in health protection? The Swedish government plans to spend approximately $1,000 per home reducing high radon levels, resulting in about $10,000 in savings per life spared. EPA estimates that the cost of remediation in most homes is less than $1,500. The cost of radon testing and mitigation per life saved compares favorably with that of other government programs.
If excessive levels of indoor radon are found in a structure, low-cost, quick-fix methods should be implemented first. These methods include limiting the amount of time spent in contaminated areas and increasing ventilation in the areas. It is wise to consult with the state radiation protection office before implementing major abatement projects. Information on methods of reduction can be obtained from several sources listed in the Suggested Reading and Sources of Information sections.
- Subslab depressurization is one of the most effective methods of lowering radon levels in many homes.
In addition to increasing ventilation, radon control measures include sealing the foundation, subslab depressurization (creating negative pressure in the soil), pressurizing the home, and using air-cleaning devices. Methods of increasing ventilation include opening windows, ventilating basements and crawl spaces, ventilating sump-holes and floor drains to the outside of the house, and increasing air movement with ceiling fans. Ventilation must be modified properly, however, because increased ventilation can depressurize the house in some cases, causing an increase of soil gas entry to the home. Heat exchangers provide a way of bringing fresh air indoors without major heat loss, but these must be properly balanced or they can worsen the problem.
Preventing soil gas entry is more important than increasing whole-house ventilation. Prevention of soil gas entry involves sealing the foundation and depressurizing the soil. Potentially useful methods for prevention of soil gas entry include using vapor barriers around the foundation, sealing cracks and holes with epoxies and caulks, and sealing the crawl space from the rest of the house. Subslab depressurization can reduce radon levels by as much as 99%. Suction puts the soil at a lower pressure than the inside of the home, preventing inward migration of soil gas. Subslab depressurization involves sinking ventilation pipes below the foundation and continuously pumping air out. The cost to install subslab depressurization in an existing home is approximately $1,000 to $2,500; annual utility costs are about $100. The state radon office can be consulted to obtain a listing of radon mitigation contractors that have passed the EPA Radon Contractor Proficiency program. If the equipment is installed during construction of the home, however, the cost of subslab depressurization is considerably less; it is much easier to install pipes during construction than to retrofit later. Physicians and other health professionals can perform a public service by becoming acquainted with local building codes and urging local jurisdictions to include the installation of capped pipes terminating in a space under the foundation to allow for later subslab depressurization if needed.
Pipes, attached to a suction fan, are inserted into the ground below the basement floor, creating a low-pressure region under the house. Adapted from Brenner (1989).
Standards and Regulations
- No enforceable regulations exist to control indoor radon levels—only guidelines and a national goal.
No regulations mandate specific mimimum radon exposure levels for indoor residential and school environments—only guidelines for remediation, such as the EPA recommendations and a national goal. EPA based its guidelines not only on risk considerations, but also on technical feasibility. No level at which the risk of exposure to alpha emitters is zero is thought to exist. Many standards and guidelines for radon are being reviewed (Table 3 and Table 4), and changes might occur over time. EPA or state health departments should therefore be consulted for the most up-to-date standards.
- The national goal is for indoor radon levels to be as low as those outdoors. About 0.4 pCi/L radon is normally found in outside air.
In October 1988, the Indoor Radon Abatement Act was passed. This act states that the "national long-term goal of the United States with respect to radon levels in buildings is that the air within buildings in the United States should be as free of radon as the ambient air outside of buildings." The act mandates that EPA update its publication, A Citizen's Guide to Radon, and provide a series of action levels indicating the health risk associated with these various levels. The guide will also provide information on the risk to sensitive populations, testing methods, and the cost and feasibility of mitigation techniques. EPA recommends remediation for homes and other buildings with levels above 4 pCi/L, with the caveat that corrective action be taken below this level on a case-by-case basis.
Table 3. Residential Standards and Regulations for Radon
| Source | Focus | Level* | Comments |
|---|---|---|---|
| Indoor Radon Abatement Act | Indoor air (residential) | Indoor = outdoor (~0.4 pCi/L) | National goal |
| National Council for Radon Protection | Indoor air (residential) | 8 pCi/L | Guideline |
| U.S. Environmental Protection Agency | Indoor air (residential) | 4 pCi/L | Current action level |
| Schools | 4 pCi/L† | Guideline for action | |
| Water | 4,000 pCi/L with state indoor air risk reduction program | Proposed regulation | |
| 300 pCi/L without state indoor air risk reduction program | |||
| *pCi/L: picocuries per liter. †The U.S. Environmental Protection Agency recommends action below 4 pCi/L in schools on a case-by-case basis. | |||
Table 4. Occupational Standards and Regulations for Radon
| Source | Focus | Level | Comments |
|---|---|---|---|
| National Institute for Occupational Safety and Health | Occupational (mining) | 1 WLM */year and ALARA† | Advisory; exposure limit |
| Occupational Safety and Health Administration | Occupational | 4 WLM/year | Regulation |
| Mine Safety and Health Administration | Mining | 4 WLM/year | Regulation |
| American Conference of Governmental Industrial Hygienists | Occupational | 4 WLM/year | Advisory for radon daughters |
| *WLM (working-level month): a unit of measure commonly used in occupational environments. (Because WLM bears a complex relationship to picocuries per liter, physicians with responsibility for mine workers are urged to contact the National Institute for Occupational Safety and Health or the U.S. Environmental Protection Agency for further information.) †ALARA: as low as reasonably achievable. | |||
Radon Toxicity
Sources of Information
More information on the adverse effects of radon and the treatment and management of persons exposed to radon can be obtained from the Agency for Toxic Substances and Disease Registry (ATSDR), your state and local health departments, and university medical centers. Physicians and other health professionals can obtain materials from EPA for display purposes. EPA maintains a radon hotline (1-800-SOS-RADON).
Case Studies in Environmental Medicine: Radon Toxicity is one of a series. For other publications in this series, use the order form on page 34. For clinical inquiries, contact ATSDR, Division of Toxicology and Environmental Medicine, at 770-488-3490.
State Radon Contacts
Congress has mandated that each state set up an office to deal with requests for radon testing and remedial action. Note that the 800 numbers are for in-state use only and are subject to change. An updated list is available from URL http://www.epa.gov/radon/whereyoulive.html.
Native Americans living on Indian lands should contact their Tribal Health Department of Housing Authority for assistance. (See Tribal Radon Program Offices information.)
| Alabama 1-800-582-1866 334-206-5391 | Idaho 1-800-445-8647 208-332-7319 | Minnesota 1-800-798-9050 651-215-0909 |
| Alaska 1-800-478-8324 | Illinois 1-800-325-1245 217-785-9958 | Mississippi 1-800-626-7739 601-987-6893 |
| Arizona 602-255-4845, x244 | Indiana 1-800-272-9723 317-233-7147 | Missouri 1-800-669-7236 572-751-6160 |
| Arkansas 1-800-482-5400 501-661-2301 | Iowa 1-800-383-5992 515-281-4928 | Montana 1-800-546-0483 406-444-6768 |
| California 1-800-745-7236 916-324-2208 | Kansas 1-800-693-5343 785-296-1561 | Nebraska 1-800-334-9491 402-471-0594 |
| Colorado 1-800-846-3986 303-692-3090 | Kentucky 502-564-4856 | Nevada 775-687-5394, x275 |
| Connecticut 860-509-7367 | Louisiana 1-800-256-2494 225-925-7042 | New Hampshire 1-800-852-3345, x4674 603-271-4674 |
| Delaware 1-800-464-4357 302-739-4731 | Maine 1-800-232-0842 207-287-5676 | New Jersey 1-800-648-0394 |
| District of Columbia 202-535-2999 | Maryland 1-800-438-2472 x2086 215-814-2086 | New Mexico 505-827-4300 |
| Florida 1-800-543-8279 850-245-4288 | Massachusetts 1-800-RADON95 [1-800-823-6695] 413-586-7525 x1124 | New York 1-800-458-1158 |
| Georgia 1-800-745-0037 404-872-3549 | Michigan 1-800-723-6642 517-335-8037 | North Carolina 919-571-4141 |
| Hawaii 808-586-4700 | Texas 512-834-6688 | North Dakota 701-221-5188 |
| Oklahoma 405-271-5221 | Utah 801-538-6734 | Ohio 1-800-523-4439 |
| Oregon 503-731-4014 | Vermont 1-800-640-0601 | Guam 671-475-1611 |
| Pennsylvania 1-800-237-2366 | Virginia 1-800-468-0138 | Puerto Rico 787-274-7815 |
| Puerto Rico 809-767-3563 | Washington 1-800-323-9727 | Virgin Islands 212-637-4013 |
| Rhode Island 401-277-2438 | West Virginia 1-800-922-1255 | Tribal Radon Program Offices |
|---|---|---|
| South Carolina 1-800-768-0362 | Wisconsin 608-267-4795 | Hopi Tribe Arizona: 520-734-2442 x635 |
| South Dakota 605-773-3351 | Wyoming 1-800-458-5847 | Inter-Tribal Council of Arizona: 602-307-1527 |
| Tennessee 1-800-232-1139 | Navajo Nation: 520-871-7863 | |
| Duckwater Shoshone-Paiute Tribe: 702-863-0222 (Nevada) |
State Radon Web Sites
- Alabama Geological Survey- Radon
- Arizona Geological Survey - Radon Information http://www.azgs.az.gov/hazards_radon.shtml
- California Department of Health Services - Indoor Radon
- Colorado Department of Public Health and Environment (CDPHE) - Indoor Radon http://www.cdphe.state.co.us/lr/Radon/rn_hom.asp
- Connecticut Department of Public Health Radon Program http://www.dph.state.ct.us/BRS/radon/radmain.htm
- Florida Bureau of Environmental Toxicology - Radon Home Page http://www.doh.state.fl.us/environment/facility/radon/index.html
- Idaho - Facts About Radon http://www2.state.id.us/dhw/BEHS/radon.htm
- Illinois Dept. of Nuclear Safety http://www2.state.il.us/idns/html/radon/radon.asp
- Indiana State Department of Health - Radon
- Iowa Department of Public Health - Radon http://www.idph.state.ia.us/radoniniowa.asp
- Kansas Department of Health and Environment - Radiation Section http://www.kdhe.state.ks.us/radiation/
- Kentucky Cabinet for Health Services Department for Public Health - Radon Gashttp://chfs.ky.gov/dph/info/phps/radongas.htm
- Louisiana State Radon Web Site http://www.deq.state.la.us/laboratory/rpradon.htm
- Maine Radon Homepage http://www.state.me.us/dhs/eng/rad/hp_radon.htm
- Maryland Geological Survey http://www.mgs.md.gov/esic/brochures/radon.html
- Massachusetts Department of Public Health - Public Health Fact Sheet - Radon exposure-topics/radiation/
- Michigan Dept. of Environmental Quality - Drinking Water and Radiological Protection Division http://www.michigan.gov/deq/0,1607,7-135-3313_3675---S,00.html
- Minnesota Department of Health - Radon in Minnesota Homes http://www.health.state.mn.us/divs/eh/indoorair/radon/index.html
- Mississippi State Department of Health - Radon http://www.msdh.state.ms.us/msdhsite/index.cfm/11,0,100,html
- Missouri Department of Health and Senior Services - Radon Program http://health.mo.gov/living/environment/radon/
- Montana Department of Environmental Quality- Planning, Prevention and Assistance Division - Radon and You: Promoting Public Awareness of Radon in Montana's Air and Ground Water http://www.mbmg.mtech.edu/radon.htm
- Nebraska Health & Human Services - Radon http://www.hhs.state.ne.us/enh/radon/radon.htm
- Nevada Radiological Health Section - Radon http://health2k.state.nv.us/bhps/rhs/srha.htm
- New Hampshire Department of Health and Human Service - Radon pdf overview http://www.dhhs.nh.gov/dphs/cdcs/hom/documents/hom-radon.pdf
- New Jersey Dept. of Environmental Protection - Radon Section http://www.state.nj.us/dep/rpp/radon/index.htm
- New Mexico Environmental Department - Indoor Radon Outreach Program http://www.nmenv.state.nm.us/nmrcb/radon.html
- New York - RX for Radon http://www.health.state.ny.us/nysdoh/radon/radonhom.htm
- Radon in North Carolina http://www.ces.ncsu.edu/depts/fcs/radon/
- North Dakota Department of Health - Radon http://www.ndhealth.gov/aq/iaq/Radon/index.htm
- Ohio Radon Information System http://www.radon.utoledo.edu/
- Oregon Radiation Protection Services - Radon http://www.ohd.hr.state.or.us/rps/radon/index.cfm
- Pennsylvania Dept. of Environmental Protection - Radon Division
- South Dakota Dept. of Environment and Natural Resources - Radon http://denr.sd.gov/des/aq/aarad.aspx
- Tennessee - Radon Program http://www.state.tn.us/environment/apc/radon/
- Utah Dept. of Environmental Quality - Indoor Radon Program http://www.eq.state.ut.us/eqrad/RADON.htm
- Vermont - Dept. of Health Radon Education Program http://healthvermont.gov/enviro/rad/Radon.aspx
- Virginia Virginia Radiation Protection Programs Indoor Radon Program
- Washington State Department of Ecologyhttp://www.ecy.wa.gov/pubs/96503/appd.htm
- West Virginia Radon Program http:www.wvdhhr.org/rtia/pdf/radon%20facts.pdf
- Wisconsin - Radon Program http://www.dhfs.state.wi.us/dph_beh/RadonProt/index.htm
- Wyoming Radon Project http://wdhfs.state.wy.us/radon/
Radon Toxicity
Suggested Reading
General
- Anonymous. 1986. Standard procedures for radon measurement developed by the EPA. J Environ Health 49:163-5.
- Bierma TJ. 1989. Radon risk factors. J Environ Health 51:277-81.
- Brenner DJ. 1989. Radon risk and remedy. New York: W.H. Freeman and Co.
- Council on Scientific Affairs. 1987. Radon in homes. JAMA 258:668-72.
- Kerr RA. 1988. Indoor radon: the deadliest pollutant. Science 240:606-8.
- National Research Council. 1999. Health effects of exposure to radon, BEIR VI. Washington (DC): National Academy Press. Available from URL: books.nap.edu/books/0309056454/html/index.html.
- National Council on Radiation Protection and Measurements. 1984. Evaluation of occupational and environmental exposures to radon and radon daughters in the United States. Bethesda (MD): National Council on Radiation Protection and Measurement. NCRP report no. 78.
- Nero AV, Schwehr MB, Nazaroff WW, Revzan KL. 1986. Distribution of airborne radon-222 concentrations in U.S. homes. Science 234:992-7.
- Nazaroff WW, Nero AV Jr, editors. 1988. Radon and its decay products in indoor air. New York: Wiley.
- Lubin JH. 1988. Models for the analysis of radon-exposed populations. Yale J Biol Med 61:195-214.
Health Effects
- Harley N, Samet JM, Cross FT, Hess T, Muller J, Thomas D. 1986. Contribution of radon and radon daughters to respiratory cancer. Environ Health Perspect 70:17-22.
- Samet JM, Nero AV Jr. 1989. Sounding board: indoor radon and lung cancer. N Engl J Med 320:591-4.
Related Documents
- Agency for Toxic Substances and Disease Registry. 1990. Toxicological profile for radon. Atlanta: US Department of Health and Human Services.
- American Conference of Governmental Industrial Hygienists. 1999. Threshold limit values for chemical substances and physical agents and biological exposure indices. Cincinnati (OH): American Conference of Governmental Industrial Hygienists.
- Centers for Disease Control. 1985. Health hazards associated with elevated levels of indoor radon—Pennsylvania. MMWR 34:6578.
- Centers for Disease Control. 1987. A recommended standard for occupational exposure to radon progeny in underground mines. Atlanta: US Department of Health and Human Services. Report No. (NIOSH): 88-101. Available from URL: http://www.cdc.gov/niosh/88-101.html.
- Centers for Disease Control. 1989. Radon exposure assessment—Connecticut. MMWR 38:713-5.
- Centers for Disease Control. 1989. Lung cancer and exposure to radon in women New Jersey. MMWR 38:715-8.
- US Environmental Protection Agency. 1986. Radon reduction techniques for detached houses: technical guidance. 2nd ed. Washington (DC): US Environmental Protection Agency, Office of Research and Development. Report No. EPA 625/587/019.
- US Environmental Protection Agency. 1987. Radon reference manual. Washington (DC): US Environmental Protection Agency, Office of Radiation Programs. Report No. EPA 520/18720.
- US Environmental Protection Agency. 1987. Removal of radon from household water. Washington (DC): US Environmental Protection Agency, Office of Research and Development. Report No. EPA87011.
- US Environmental Protection Agency. 1989. Radon measurements in schools: an interim report. Washington (DC): US Environmental Protection Agency, Office of Radiation Programs. Report No. EPA 520/189/010.
- US Environmental Protection Agency. 1989. Radon reduction methods: a homeowner's guide. 3rd ed. Washington (DC): US Environmental Protection Agency, Office of Research and Development. Report No. EPA89005.
- US Environmental Protection Agency. 1992. A citizen's guide to radon: the guide to protecting yourself and your family from radon. 3rd ed. Washington (DC): US Environmental Protection Agency, Office of Air and Radiation. Report No. OPA86004. Available from URL: www.epa.gov/iaq/radon/pubs/citguide.html. Also available in Spanish from URL: www.epa.gov/iaq/radon/pubs/elradon.html.
- US Environmental Protection Agency. 1992. Consumer's guide to radon reduction: how to reduce radon levels in your home. Washington (DC): US Environmental Protection Agency, Office of Air and Radiation. Available from URL: www.epa.gov/iaq/radon/pubs/consguid.html.
- US Environmental Protection Agency. 1993. Radon - A physician's guide. Washington (DC): US Environmental Protection Agency, Office of Air and Radiation. Available from URL: www.epa.gov/iaq/radon/pubs/physic.html.
- US Environmental Protection Agency. 2000. Radon in water. Washington (DC): US Environmental Protection Agency, Office of Radiation Programs. Available from URL: www.epa.gov/iaq/radon/rnwater.html.
- US Environmental Protection Agency. The national radon measurement proficiency (RMP) program: cumulative proficiency report. Washington (DC): US Environmental Protection Agency, Office of Radiation Programs. Report No. EPA 520/188/024. (Published twice annually for various states; lists participating vendors of radon detection equipment and services.)
- Public Health Service. The health consequences of smoking: cancer. A report of the Surgeon General. Washington (DC): US Department of Health and Human Services; 1982. DHHS report no. (PHS) 8250179.
1.11 Complete Radon MSDS and Toxicology Information for RADON Gas
CASRN: 10043-92-2
CONTENTS:
Human Health EffectsEvidence for Carcinogenicity
Human Toxicity Excerpts
Medical Surveillance
Populations at Special Risk
Probable Routes of Human Exposure
Animal Toxicity Studies
Evidence for Carcinogenicity
Non-Human Toxicity Excerpts
Metabolism/Pharmacokinetics
Absorption, Distribution & Excretion
Biological Half-Life
Interactions
Pharmacology
Therapeutic Uses
Interactions
Environmental Fate & Exposure
Probable Routes of Human Exposure
Natural Pollution Sources
Environmental Fate
Soil Adsorption/Mobility
Environmental Water Concentrations
Sediment/Soil Concentrations
Atmospheric Concentrations
Other Environmental Concentrations
Environmental Standards & Regulations
CERCLA Reportable Quantities
Atmospheric Standards
State Drinking Water Guidelines
Chemical/Physical Properties
Molecular Formula
Molecular Weight
Color/Form
Odor
Taste
Boiling Point
Melting Point
Critical Temperature & Pressure
Density/Specific Gravity
Heat of Vaporization
Solubilities
Spectral Properties
Vapor Pressure
Viscosity
Other Chemical/Physical Properties
Chemical Safety & Handling
Hazardous Reactivities & Incompatibilities
Protective Equipment & Clothing
Preventive Measures
Shipment Methods and Regulations
Storage Conditions
Cleanup Methods
Disposal Methods
Manufacturing/Use Information
Major Uses
Methods of Manufacturing
General Manufacturing Information
Laboratory Methods
Analytic Laboratory Methods
Special References
Special Reports
Synonyms and Identifiers
Related HSDB Records
Synonyms
Associated Chemicals
Evidence for Carcinogenicity:
Evaluation: There is sufficient evidence for the carcinogenicity of radon and its decay products in experimental animals. There is sufficient evidence for the carcinogenicity of radon and its decay products in humans. Overall evaluation: Radon and its decay products are carcinogenic to humans (Group 1).
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 241 (1988)]**PEER REVIEWED**
Human Toxicity Excerpts:
The influence of radon and radon daughters on development of respiratory cancer is reviewed. Epidemiological studies thus far indicate that excess lung cancer mortality is connected with miners having cumulative radon daughter exposures somewhat below 100 working level month. A working level month is defined as a 170 hr working month exposure to alpha radiation from radon daughters equal to 1.3X10+5 megaelectron volts emitted in 1 liter of air. An additive rather than a multiplicative model has been gaining support to illustrate the connection between smoking and radon daughter induced lung cancer.
[Harely N et al; Environmental Health Perspectives 70: 17-21 (1986)]**PEER REVIEWED**
A case referent study on the possible association between radon emanating from the ground and bronchial cancer was carried out on 292 female lung cancer cases and 584 matched population referents. Both groups had lived for at least 30 yr in the city of Stockholm, Sweden. The cases were diagnosed during 1972 to 1980 with oat cell and other types of anaplastic pulmonary carcinomas. A sample of about 10% of the dwellings where cases and referents had lived was selected for measurements of radon and radon daughters. The measurements indicated increased radon daughter concentrations in ground level dwellings within radon risk areas where lung cancer cases had lived, suggesting that this exposure was of etiologic importance.
[Svensson C et al; Int Arch Occup Environ Health 59 (2): 123-31 (1986)]**PEER REVIEWED**
Indoor radon concentrations seem to depend on both building material and leakage of radon from the ground. This study, in a rural area, is a further attempt to elucidate the etiology of lung cancer, taking into consideration type of house and ground conditions, as well as smoking habits. Although the choice of a rural study population helped to eliminate various confounding exposures in the urban environment, it limited the size of the study because of the rareness of lung cancer in rural populations. Long term residents, 30 yr or more in the same houses, were studied, and again an association was found between lung cancer and estimated exposure to radon and radon daughters in homes. The data also seem to indicate the possibility of a multiplicative effect between smoking and exposure to radon and radon daughters in homes, but there was also some confounding between these factors in the data.
[Edling C; Scand J Work Environ Health 10 (1): 25-34 (1984)]**PEER REVIEWED**
The chief hazard is inhalation of the gaseous element and its solid daughters, which are collected on the normal dust of the air. This material is deposited in the lung and has been considered to be a major causative agent in the high incidence of lung cancer.
[Sax, N.I. Dangerous Properties of Industrial Materials. 6th ed. New York, NY: Van Nostrand Reinhold, 1984., p. 2357]**PEER REVIEWED**
Peripheral lymphocyte chromosomes from 80 underground uranium miners and 20 male controls in the Colorado plateau, USA, were studied, taking into account confounding factors such as smoking habits and diagnostic radiation. Five groups with increasing cumulative exposure to radon and radon decay products were selected. Peripheral lymphocytes were cultured for 68-72 hr. Pericentric inversions and translocations showed the most consistent pattern of increase with estimated radiation dose. All aberration categories, except dicentrics and rings, demonstrated a significant, uniform increase with dose from < 100 to 1740-2890 working level month, but not at >3000 working level month. Significantly more chromosomal aberrations were observed among workers with markedly atypical bronchial cell cytology, suspected carcinoma, or carcinoma in situ than among miners with regular or mildly atypical cells, as evaluated by sputum cell cytology.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 212 (1988)]**PEER REVIEWED**
A case control study was carried out in Port Hope, Ontario, Canada, to evaluate the relative significance of domestic exposure to radon (Rn) in the etiology of lung cancer over a period of 10 years, with control for the effect of smoking. Twenty seven cases of lung cancer and 49 comparisons matched for age and duration of residence in the town were analyzed. Examination of the histopathological records revealed that 11 of the 27 cases (40.7%) had squamous cell carcinoma and six had adenocarcinoma (22.6%); the other ten cases were not classified. After allowing for the effect of smoking, a marginally significant association (degree of significance equal to 0.057) was established between exposure to Rn and lung cancer. Classification of exposure in terms of living or not living in a problem home demonstrated a strong confounding between Rn exposure and smoking, in that all four exposed cases were smokers while the two exposed comparisons were not. In this case also, after allowing for the effect of smoking, a marginally significant association (significance 0.050) was established between Rn exposure and lung cancer. About 90% of all lung cancer cases identified demonstrated a strong association with cigarette smoking.
[Lees REM et al; Inter J Epidemiol 16 (1): 7-12 (1987)]**PEER REVIEWED**
Uranium miners in Saskatchewan. Mean time of follow after start of work: 14 yr cut-off date for follow up: 12/31/80. Numbered studied: 8,487. Mean age at first exposure: 28 yr. Mean calendar year of first exposure: 1966. Mean exposure: 2.8 WLM for surface workers and 16.6 WLM for underground workers. Control data were taken from Canadian national male rates. Radon progeny measurements were made from 1954 to 1967. Radon gas measurements were made from 1954 to 1967. Uranium mining began in 1949 and ended in 1982. Workers with other mining experience were excluded from analysis. At exposure levels greater than 100 working level months, the number of observed cases of lung cancer, 17, was significantly greater than the expected number of 2.21 (p < 0.05). Lung cancer risk appeared to be a function of age at first exposure. Information on smoking habit was not reported.
[Howe GR et al; JNCI 77: 357-62 (1986) as cited in IL Department of Energy and Natural Resources; Risk Assessment of Exposure to Waterborne and Airborne Radon-222 in IL p.28 (1987) ILENR/RE-AQ-87/21]**PEER REVIEWED**
... The histopathological patterns of lung cancer in uranium miners in the Colorado plateau region /are described /. The cases were miners included in the US Public Health Service study and other miners who lived in the Colorado plateau area. The classification of the histopathology was based on either a single pathologist's reading or on the consensus of a panel; 312 cases of lung cancer were analyzed among uranium miners. Most of the cases occurred in cigarette smokers; the series included 14 nonsmokers. In the early reports, the majority of the cases were small cell carcinomas; however, the proportion of this cell type declined from 76% in 1954 to 22% (compared to 17% in non-mining cigarette smokers) in the late 1970s. In nonsmokers, eight cases were small cell carcinomas and the remaining six were of other cell types.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 236 (1988)]**PEER REVIEWED**
In all situations where an excess of lung cancer has been observed, there have been simultaneous exposure to other potentially carcinogenic substances or agents such as other metals ... or radon.
[Zenz, C., O.B. Dickerson, E.P. Horvath. Occupational Medicine. 3rd ed. St. Louis, MO., 1994, p. 604]**PEER REVIEWED**
Lung cancer is the only malignancy clearly associated with exposure to radon.
[Zenz, C., O.B. Dickerson, E.P. Horvath. Occupational Medicine. 3rd ed. St. Louis, MO., 1994, p. 409]**PEER REVIEWED**
... A higher incidence of chromosomal aberrations /was reported/ among uranium miners exposed to radon and radon daughters at cumulative exposures ranging from less than 100 to more greater than 3,000 WLM, a compared to their matched controls. A clear exposure related increase was observed for the groups exposed to 770 to 2,890 WLM with a sharp decrease at the highest dose group (greater than 3,000 WLM).
[Brandom W et al; Radiat Res 76: 159-171 (1978) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.23 (1990) PB91-180422]**PEER REVIEWED**
Statistically significant excesses in lung cancer deaths have been reported in uranium miners in the United States.
[Archer V et al: Health Phys 25: 351-371 (1973) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.23 (1990) PB91-180422]**PEER REVIEWED**
Among uranium miners, epidermoid, small cell undifferentiated, and adenocarcinoma were present with increased frequency, while large cell undifferentiated and other morphological types of lung cancer were seen less frequently.
[Archer V et al; Cancer 34: 2056-2060 (1974)as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.24 (1990) PB91-180422]**PEER REVIEWED**
Purpose: To clarify the relationship between domestic radon exposure and the occurrence of chromosomal aberrations, stable translocations especially, in peripheral blood lymphocytes. The study comprised a total of 84 non-smoking individuals, divided into three groups according to radon concentration measurements performed in their homes: low radon concentration (<100 Bq/cu m, mean 67 Bq/cu m), medium (200-400 Bq/cu m, mean 293 Bq/cu m) or high (>800 Bq/cu m, mean 1737 Bq/cu m). Significant correlation of translocations with age was observed, and due to the high mean age (50 years) the genome-corrected frequency of translocations was high: about one translocation in 100 metaphases. Chronic exposure to high concentrations of domestic radon did not increase the rate of stable or unstable chromosomal aberrations in peripheral blood lymphocytes detected by FISH chromosome painting. A strong age effect was observed.
[Lindholm C et al; International Journal of Radiation Biology 75 (8): 921-8 (1999)]**PEER REVIEWED**
This study investigated residential radon exposure and lung cancer risk, using both standard radon dosimetry and a new radon monitoring technology that, evidence suggests, is a better measure of cumulative radon exposure. Missouri women (aged 30 to 84 years) newly diagnosed with primary lung cancer during the period January 1, 1993, to January 31, 1994, were invited to participate in this population-based case-control study. Both indoor air radon detectors and CR-39 alpha-particle detectors (surface monitors) were used. When surface monitors were used, a significant trend in lung cancer odds ratios was observed for 20-year time-weighted-average radon concentrations. When surface monitors were used, but not when standard radon dosimetry was used, a significant lung cancer risk was found for radon concentrations at and above the action level for mitigation of houses currently used in the United States (148 Bqm-3). The risk was below the action level used in Canada (750 Bqm-3) and many European countries (200-400 Bqm-3).
[Alavanja MC et al; Am J Public Health 89 (7): 1042-8 (1999)]**PEER REVIEWED**
Medical Surveillance:
A preplacement medical examination of each miner shall include the following: 1. A comprehensive medical and work history (including smoking history) that emphasizes the identification of existing medical conditions and attempts to elicit information about previous occupational exposure to radon progeny. 2. A thorough examination of the miner's respiratory system, including pulmonary function tests. The initial and subsequent vital capacity and forced expiratory volume in 1 second using the current American Thoracic Society recommendations on instrumentation, technician training and interpretation. A prospective miner with symptomatic, spirometric, or radiographic evidence of pulmonary impairment should be counseled about the risks of continued exposure. 3. A posterio-anterior chest x-ray using the current American Thoracic Society recommendations on instrumentation, technician training, and interpretation. 4. Other tests deemed appropriate by the physician.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.5 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
Periodic medical examination for each miner shall include the following: 1. An annual update of medical and work histories (including smoking history). 2. An evaluation of the miner's respiratory system. Because of the potential for chronic respiratory disease, this evaluation shall include spirometry at intervals determined by the physician. Miners that have spirometric or radiographic evidence or symptoms of pulmonary impairment should be counseled by the physician regarding the risks of continued exposure. 3. A posterior-anterio chest x-ray at intervals determined by the physician using the current American Thoracic Society recommendations on instrumentation, technician training and interpretation. Periodic chest x-rays are recommended for monitoring miners exposed to fibrogenic respiratory hazards. Ordinarily, chest x-rays may be obtained every 5 years for the first 15 years of employment and every 2 years thereafter, depending on the nature and intensity of exposures and their related health risks. A recent x-ray obtained for other purposes may be substituted for the periodic x-ray if it is of acceptable quality.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.5 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
The mine operator shall retain all records of the monitoring. All monitoring records shall be retained for at least 40 years after termination of employment.
[NIOSH; Criteria for a recommended standard, occupational exposure to radon progeny in underground mines p.14 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Whenever medical surveillance is indicated, in particular when exposure to a carcinogen has occurred, ad hoc decisions should be taken concerning ... /cytogenetic and/or other/ tests that might become useful or mandatory. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 23]**PEER REVIEWED**
Populations at Special Risk:
Special groups which seem to be at particular risk from radon daughters include smokers or individuals with pulmonary disease.
[Harely N et al; Environmental Health Perspectives 70: 17-21 (1986)]**PEER REVIEWED**
Probable Routes of Human Exposure:
... water supplies to the building.
[Doull, J., C.D.Klassen, and M.D. Amdur (eds.). Casarett and Doull's Toxicology. 3rd ed., New York: Macmillan Co., Inc., 1986., p. 676]**PEER REVIEWED**
The extent to which the population is exposed to (222)radon and its daughters in the air, especially indoors, has recently received increased attention. Levels of indoor (222)radon and daughter concentrations arise from several sources in addition to entering from the outside air. They include building materials and the soil and rock underlying the building. The level in homes may also be affected by the ventilation rate, which, due to energy conservation measures, is generally being decreased in houses in the United States.
[Klaassen, C.D., M.O. Amdur, Doull J. (eds.). Casarett and Doull's Toxicology. The Basic Science of Poisons. 5th ed. New York, NY: McGraw-Hill, 1995., p. 862]**PEER REVIEWED**
Radon gas has been implicated in the occurrence of lung cancer in individuals engaged in mining ores.
[Klaassen, C.D., M.O. Amdur, Doull J. (eds.). Casarett and Doull's Toxicology. The Basic Science of Poisons. 5th ed. New York, NY: McGraw-Hill, 1995., p. 789]**PEER REVIEWED**
Persons working with radium and its cmpd are also exposed to radon.
[International Labour Office. Encyclopedia of Occupational Health and Safety. Vols. I&II. Geneva, Switzerland: International Labour Office, 1983., p. 1896]**PEER REVIEWED**
Animal Toxicity Studies:
Evidence for Carcinogenicity:
Evaluation: There is sufficient evidence for the carcinogenicity of radon and its decay products in experimental animals. There is sufficient evidence for the carcinogenicity of radon and its decay products in humans. Overall evaluation: Radon and its decay products are carcinogenic to humans (Group 1).
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 241 (1988)]**PEER REVIEWED**
Non-Human Toxicity Excerpts:
1,800 specific pathogen free Sprague-Dawley rats were exposed to radon progeny for 1-3 hr/day for 14-82 days, yielding an accumulated exposure of 20-50 working level months. An additional 600 rats were unexposed. The lung cancer incidence in rats was reported to be directly proportional to their lifetime cumulative exposure to radon progeny. ... The amount of radiation needed to double the natural incidence of lung cancer in these rats was 20 working level months. Reduced life spans were not observed for rats in any of the exposure groups.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.35 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
A group of 12 male SPF Sprague-Dawley rats, weighing 200-250 g, was exposed once to an aerosol of cerium hydroxide dust (chemical and physical characteristic and particle concentration unspecified); lung retention per animal was estimated to be 0.5-1.0 mg. The animals were subsequently exposed to radon at a concentration of 7.5X10-7 Ci/l (27.8X10+6 Becquerel/cu m) for 5 hr per day on three days per week for a total of 540 hr over a period of approximately ten months. Exposure to radon was produced by passing air over a finely ground ore containing about 25% uranium and circulating it into the inhalation chamber. A second group of 20 rats (presumably of the same strain and weight) was exposed only to 7.5X10-7 Ci/l (27.8X10+6) Becquerel/cu m radon for 5 hr per day on five days per week for a total of 620 hr. Two control groups (number, weight, sex, and strain unspecified) were untreated or were exposed to cerium hydroxide only. Animals were killed when moribund. ... All of the rats still alive in the eleventh month after the beginning of the experiment had pulmonary cancers. There was no clear statement of tumor incidences in the experimental groups. In the group exposed to cerium hydroxide and radon, 3/12 rats died before the 11th month; thus, presumably, nine developed lung cancers. In the group exposed to radon only, seven animals died of infection before the 11th month, and in three of these that could not be autopsied, clear evidence of lung cancer had been see on previous x-rays; thus, presumably, 16 rats developed lung cancers. All tumors were described as invasive, mixed adenosquamous carcinomas. Extrapulmonary metastases occurred in one animal only. Most or all of the tumors were believed to be bronchiolar or bronchiolo-alveolar in origin.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 198 (1988)]**PEER REVIEWED**
Male Sprague-Dawley rats, three months old at the beginning of the experiment, were used to study the effects of low doses of radon on lung cancer incidence. Groups of 500 rats were exposed to a total dose of 20 or 40 working level month by inhalation, and 600 rats were used as controls. Animals were exposed twice weekly for 1 hr to 111000 Becquerel/cu m radon for 42 sessions (cumulative exposure, 20 working level month ) or for 82 sessions (cumulative exposure, 40 working level month ). Exposure levels were measured with alpha-track detectors (ISID type) commonly used in French mines. Animals were kept until moribund. Lungs were excised when gross lesions were observed, and those from 80 of the rats exposed to 20 working level month and from 91 of the rats exposed to 40 working level month were examined. The proportions of animals with lung cancer were 0.83, 2.21 and 3.82% in the control, 20 working level month and 40 working level month exposed groups, respectively; statistical analysis showed a highly significant trend (p< 0.006; one sided). The distribution of tumor types in the three groups was: one, three, and eight squamous cell carcinomas; three, five and nine adenocarcinomas; and two, three, and two bronchiolar-alveolar carcinomas. Statistical analysis of dose effects showed a significant trend for squamous cell carcinomas (p< 0.003) and for adenocarcinomas (p< 0.02) but not for bronchiolar-alveolar carcinomas. Statistically significant trends were also found for dose dependence and tumor size (p< 0.001) and for pleural invasion (p< 0.02). The first tumor at death was discovered at 782, 580, and 498 days in the control, 20 working level month and 40 working level month exposed groups, respectively. No information was given on tumors at other sites.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 200 (1988)]**PEER REVIEWED**
Groups of 102 male Syrian golden hamsters, two months old at the start of the experiment, were exposed to room air, 670 working level radon decay products, 790 working level month radon decay products with uranium ore dust (22 mg/cu m, count median diameter, 0.19-0.36 um) or uranium ore dust (19 mg/cu m). Animals were exposed simultaneously to the various treatments for 6 hr per day, on five days per week for life and were killed when moribund. No difference in mean body weight or survival was observed between groups (survival unspecified). After more than one year of exposure, animals exposed to radon decay products with uranium ore dust or to uranium ore dust alone showed evidence of pneumoconiosis, and animals in the latter group had bronchial and bronchiolar hyperplasia, squamous metaplasia and alveolar adenomatosis. During the second year, hamsters exposed to radon decay products with and without uranium ore dust showed atypical squamous metaplasia. After 16-17 months of exposure, two hamsters exposed to radon decay products and one hamster exposed to radon decay products plus uranium ore dust showed features of squamous carcinoma. ... The three animals showing these lesions also showed all stages of progression from simple basal cell hyperplasia in bronchioles to malignant tumor. (The Working Group noted the inadequate reporting of the histopathological diagnosis.)
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 201 (1988)]**PEER REVIEWED**
Male Sprague-Dawley rats were exposed to radon by inhalation at 100-6000 working level month, and samples of bone marrow were prepared at various time intervals from 100 to 750 days. An increase in the frequency of sister chromatid exchanges was observed at all doses. With the highest dose, the increase was observed 100-200 days after the end of exposure, whereas with the lower doses this effect was observed only after a delay of 500-750 days. The authors considered the increase in sister chromatid exchange frequency was not due to direct radiation damage to the DNA.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 209 (1988)]**PEER REVIEWED**
The acute lethal effects of radon and radon daughters have been studied in mice. A 30-day LD50 was estimated based on single exposure via inhalation to radon and radon daughters at a concn of 2.2x10+8 pCi/L (8.1x10+9 Bq/cu m) for 5 to 40 hours. After 40 hours of exposure, 100% of the exposed mice died within 2 weeks (cause of death was not reported), while no deaths occurred within 60 days following an exposure of 26 hours or less.
[Morken D; AMA Arch Ind Health 12: 435-438 (1955) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.18 (1990) PB91-180422]**PEER REVIEWED**
... Mice were to be exposed to 4.2x10+5 pCi radon/L of air (1.6x10+7 Bq/cu m) 150 hr/wk for life. However, by week 15 of the experiment the median lifetime of the animals had been decreased by 50%. However, the cause of this decreased lifespan was not reported. The authors then sacrificed the remaining animals (15 treated mice and 3 control mice) for purposes of histopathological examination. Tracheal effects, including thickening of the mucous membrane, inflammation of the mucous glands, and destruction of cells lining the trachea, were observed. However, the onset of these effects could not be determined.
[Morken D, Scott J; U.S. Atomic Energy Commission, Univ of Rochester UR-669 (1966) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.19 (1990) PB91-180422]**PEER REVIEWED**
Evidence of chromosomal aberrations was equivocal in an animal study. Rabbits exposed to high natural background levels of (222)radon (12 WLM) for over 28 months displayed an increased frequency of chromosomal aberrations. However, when a similar study was conducted under controlled conditions (10.66 WLM), chromosomal aberrations were not found. According to the authors, the increased chromosomal aberrations in somatic cells of rabbits exposed to natural radiation were mainly due to the gamma radiation from sources other than radon.
[Leonard A et al; Can J Genet Cytol 23: 321-326 (1981) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.23 (1990) PB91-180422]**PEER REVIEWED**
Metabolism/Pharmacokinetics:
Absorption, Distribution & Excretion:
Being /an/ inert gas, radon /is/ easily retained in the lung and absorbed by the blood. ... Radon ... daughters are easily adsorbed on solid surfaces, especially colloids and dust particles present in the atmosphere. ... Radon ... and /its/ decay products enter the body by inhalation, by ingestion, or through the skin.
[International Labour Office. Encyclopedia of Occupational Health and Safety. Vols. I&II. Geneva, Switzerland: International Labour Office, 1983., p. 1896]**PEER REVIEWED**
Radon transported by the blood reaches various tissues and organs. Since it is lipid soluble its distribution depends chiefly on the fat content of organs and tissues. It has been established that 50-90% of the radon body burden is located in the fatty tissues. In a state of equilibrium 1 cu m of fatty tissue contains 45% of the quantity of radon present in 1 cu m of inhaled environmental air. Radon daughters taken in become localized largely in active deposits in the lungs, to which they represent a grave threat. Short lived and long lived radon daughters, produced within the body, may become selectively deposited in various organs. The major threat, however, is to the kidneys. ... Radon is eliminated mainly in exhaled air (about 90% in the first hour and the remainder in 6-7 hr) whereas radon daughters are eliminated mainly by excretion in feces and urine.
[International Labour Office. Encyclopedia of Occupational Health and Safety. Vols. I&II. Geneva, Switzerland: International Labour Office, 1983., p. 1896]**PEER REVIEWED**
Gases and vapors known to be absorbed (or excreted) by the skin include ... radon ... .
[Hayes, W.J., Jr., E.R. Laws Jr., (eds.). Handbook of Pesticide Toxicology Volume 1. General Principles. New York, NY: Academic Press, Inc., 1991., p. 139]**PEER REVIEWED**
The presence of radon is associated with an increase in the occurrence of lung cancer due to the deposition of radioactive substances in the bronchial region.
[International Labour Office. Encyclopaedia of Occupational Health and Safety. 4th edition, Volumes 1-4 1998. Geneva, Switzerland: International Labour Office, 1998., p. 44.10]**PEER REVIEWED**
Following ingestion of radon dissolved in water, greater than 90% of the absorbed radon was eliminated by exhalation within 100 minutes. By 600 minutes, only 1% of the absorbed amount remained in the body.
[Hursh J et al; Health Phys 11: 465-476 (1965) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.35 (1990) PB91-180422]**PEER REVIEWED**
Experiments in animals have reported the retention of radon after exposure by the intraperitoneal and intravenous routes. After intravenous administration , 1.6% to 5.0% of the administered activity was retained in the animals after 120 minutes. Retention was greatest after intraperitoneal administration at 120 minutes, but by 240 minutes it was nearly the same for both routes of administration.
[Hollcroft J, Lorenz E; Nucleonics 9: 63-71 (1949) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.36 (1990) PB91-180422]**PEER REVIEWED**
Within 24 hr, 4.5% of the radon, which was applied as a salve to intact human skin, was eliminated by exhalation, while 10% was exhaled after application of the radon to an open wound.
[Lange K, Evans R; Radiology 48: 514-516 (1947) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.36 (1990) PB91-180422]**PEER REVIEWED**
Based on the time-course of radon elimination in expired air, it appears that the majority of radon absorption following ingestion in water occurs in the stomach and small intestine, and only 1% to 3% of the ingested radon remains to enter the large intestine to be available for absorption.
[Dundulis W et al; Health Phys 47: 243-252 (1984) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.32 (1990) PB91-180422]**PEER REVIEWED**
Fat appears to be the main storage compartment in rats following inhalation exposure. In rats following an acute exposure to radon, concentrations of radon and radon daughters were much higher in the omental fat than in any of the other tissues examined, followed by the venous blood, brain, liver, kidney, heart, muscle tissues, and testes. Radon reached equilibrium in the fat in about 6 hours compared to 1 hour in all other tissues.
[Nussbaum E, Hursh J; Science 125: 552-553 (1957) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.33 (1990) PB91-180422]**PEER REVIEWED**
Biological Half-Life:
3.823 days /(222) Radon/
[Stannard JN; Radioactivity and Health, a History p.3 (1988)]**PEER REVIEWED**
The biological half life in the blood of humans has been reported to be 18 minutes for 95% of the administered dose and 180 minutes for the remaining 5%.
[Hursh J et al; Health Phys 11: 465-476 (1965) as cited in U.S. Dept Health & Human Services/ATSDR; Toxicological Profile for Radon p.35 (1990) PB91-180422]**PEER REVIEWED**
Interactions:
Multiplicative interactions may ... be seen between initiating carcinogens, as between radon and it decay products and tobacco smoking in miners of uranium.
[International Labour Office. Encyclopaedia of Occupational Health and Safety. 4th edition, Volumes 1-4 1998. Geneva, Switzerland: International Labour Office, 1998., p. 2.14]**PEER REVIEWED**
Lifetime exposures of beagles to mixtures of radon daughters, uranium ore dust, and cigarette smoke caused significant life span shortening compared with that of controls. Mean survival time of the exposed to mixtures of radon daughters and ore dust, with or without cigarette smoke, were 4-5 yr. Mean survival times of controls and dogs exposed to smoke only were equivalent during the same period. The mean radon daughter exposure of the dogs was about 13,000 working level month. /A working level month is defined as a 170 hr working month exposure to alpha radiation from radon daughters equal to 1.3X100+5 megaelectron volts emitted in 1 liter of air./ /Radon daughters/
[National Research Council; Health Risks of Radon and Other Internally Deposited Alpha-Emitters p.436 (1988)]**PEER REVIEWED**
Pharmacology:
Therapeutic Uses:
Medicine (cancer treatment) /Former use/
[Sax, N.I. and R.J. Lewis, Sr. (eds.). Hawley's Condensed Chemical Dictionary. 11th ed. New York: Van Nostrand Reinhold Co., 1987., p. 995]**PEER REVIEWED**
Interactions:
Multiplicative interactions may ... be seen between initiating carcinogens, as between radon and it decay products and tobacco smoking in miners of uranium.
[International Labour Office. Encyclopaedia of Occupational Health and Safety. 4th edition, Volumes 1-4 1998. Geneva, Switzerland: International Labour Office, 1998., p. 2.14]**PEER REVIEWED**
Lifetime exposures of beagles to mixtures of radon daughters, uranium ore dust, and cigarette smoke caused significant life span shortening compared with that of controls. Mean survival time of the exposed to mixtures of radon daughters and ore dust, with or without cigarette smoke, were 4-5 yr. Mean survival times of controls and dogs exposed to smoke only were equivalent during the same period. The mean radon daughter exposure of the dogs was about 13,000 working level month. /A working level month is defined as a 170 hr working month exposure to alpha radiation from radon daughters equal to 1.3X100+5 megaelectron volts emitted in 1 liter of air./ /Radon daughters/
[National Research Council; Health Risks of Radon and Other Internally Deposited Alpha-Emitters p.436 (1988)]**PEER REVIEWED**
Environmental Fate & Exposure:
Probable Routes of Human Exposure:
... water supplies to the building.
[Doull, J., C.D.Klassen, and M.D. Amdur (eds.). Casarett and Doull's Toxicology. 3rd ed., New York: Macmillan Co., Inc., 1986., p. 676]**PEER REVIEWED**
The extent to which the population is exposed to (222)radon and its daughters in the air, especially indoors, has recently received increased attention. Levels of indoor (222)radon and daughter concentrations arise from several sources in addition to entering from the outside air. They include building materials and the soil and rock underlying the building. The level in homes may also be affected by the ventilation rate, which, due to energy conservation measures, is generally being decreased in houses in the United States.
[Klaassen, C.D., M.O. Amdur, Doull J. (eds.). Casarett and Doull's Toxicology. The Basic Science of Poisons. 5th ed. New York, NY: McGraw-Hill, 1995., p. 862]**PEER REVIEWED**
Radon gas has been implicated in the occurrence of lung cancer in individuals engaged in mining ores.
[Klaassen, C.D., M.O. Amdur, Doull J. (eds.). Casarett and Doull's Toxicology. The Basic Science of Poisons. 5th ed. New York, NY: McGraw-Hill, 1995., p. 789]**PEER REVIEWED**
Persons working with radium and its cmpd are also exposed to radon.
[International Labour Office. Encyclopedia of Occupational Health and Safety. Vols. I&II. Geneva, Switzerland: International Labour Office, 1983., p. 1896]**PEER REVIEWED**
Natural Pollution Sources:
It is estimated that every square mile of soil to a depth of 6 inches contains about 1 g of radium, which releases radon in tiny amounts to the atmosphere. Radon is present in some spring waters, such as those at Hot Springs, Arkansas.
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-24]**PEER REVIEWED**
The total amount of radium in the outer 10 km of the earth's crust is ... 1024 Becquerel. Most of the radon produced by decay of radium is physically attached to the radium bearing material and only a small part diffuses out into the air. Other relatively important sources of radon in air outdoors are plants, ground water, oceans, etc.
[WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.144 (1983)]**PEER REVIEWED**
Environmental Fate:
ATMOSPHERIC FATE: The diffusion rate and thereby the exhalation rate is influenced by meteorological factors such as rainfall, snowfall, freezing, and variations in atmospheric pressure. An increase in these parameters will decrease the exhalation rate. Measured values of radon exhalation rate from soil vary between about 0.0002 and 0.07 Becquerel/sq m/sec.
[WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.149 (1983)]**PEER REVIEWED**
TERRESTRIAL FATE: High porosity increases the diffusion rate. The release rate from a material depends also on its moisture content: if the moisture content is very low the radon release is decreased by the effect of re-adsorption of radon atoms on surfaces in the pores. If the moisture content increases slightly, the radon release increases up to a certain moisture content, above which the release of radon decreasing again owing to a decreasing diffusion rate in water filled pores.
[Megromi K, Mamuro; J Geophys Res 79: 3357-60 (1974) as cited in WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.148 (1983)]**PEER REVIEWED**
TERRESTRIAL FATE: The mechanism of radon release from rock, soil, and other materials is not very well understood and is probably not always the same. The main physical phenomena are recoil and diffusion of the radon atom through imperfections of the crystalline structures of the radium bearing particle followed by a secondary diffusion, which depends on the porosity of the material.
[Andrews JN, Wood DF; Applied Earth Science 81: 198-209 (1972) as cited in WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.148 (1983)]**PEER REVIEWED**
AQUATIC FATE: Uranium, thorium, radium, radon, lead, and polonium radionuclide concentrations in ground waters from the Hanford Site indicate that uranium, thorium, and radium are highly sorbed. Relative to radon, these radionuclides are low by factors of 1x10(-3) to 1x10(-6). Uranium sorption is likely due to its reduction from the hexavalent state, where it is introduced via surface waters, to the tetravalent state found in the confined aquifers. The distribution of radionuclides is very similar in all of the confined aquifiers and significantly different from the distribution observed in the unconfined and surface waters. Barium correlates well with radium over three orders of magnitude, indicating that stable element analogs may be useful for inferring the behavior of radioactive waste radionuclides in this candidate geologic repository.
[Smith MR et al; Materials Research Society Proceedings p.10 (1987)]**PEER REVIEWED**
Soil Adsorption/Mobility:
Strongly adsorbed on various surfaces.
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Environmental Water Concentrations:
Surface waters generally contain very low concentrations of radon. In a survey of 25 water systems in the USA, a population weighted average of about 685 Bacquerel/cu m was found; in only two systems were there greater than 3700 Bacquerel/cu m.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 182 (1988)]**PEER REVIEWED**
1 liter of ocean water /was found to/ contain 9X10-15 mg.
[Seiler, H.G., H. Sigel and A. Sigel (eds.). Handbook on the Toxicity of Inorganic Compounds. New York, NY: Marcel Dekker, Inc. 1988., p. 493]**PEER REVIEWED**
Sediment/Soil Concentrations:
It is estimated that every square mile of soil to a depth of 6 inches contains about 1 g of radium which releases radon in tiny amounts to the atmosphere.
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-24]**PEER REVIEWED**
Atmospheric Concentrations:
On the average, one part of radon is present to 1X10+21 part of air.
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-24]**PEER REVIEWED**
Radon concentrations in the air vary daily and seasonally. Maximal concentrations occur in late summer and minimal levels are observed in winter or spring. Generally, radon levels reach their maximum in the early morning and their minimum at noon or in the afternoon.
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 178 (1988)]**PEER REVIEWED**
6X10-14 ppm in pure dry atmosphere at sea level.
[Seiler, H.G., H. Sigel and A. Sigel (eds.). Handbook on the Toxicity of Inorganic Compounds. New York, NY: Marcel Dekker, Inc. 1988., p. 493]**PEER REVIEWED**
At ground level, the time variation of radon concentrations depends on the variation of the radon exhalation rate and of the vertical dispersion of radon. The effect of increased vertical dispersion of radon by turbulence during spring, as compared with autumn, outweighs the greater exhalation rate of radon during late spring and summer, as compared with autumn and winter. The overall effect is a seasonal aeration of the radon concentration at ground level with a minimum in the spring and summer and a maximum in the autumn and winter observed in several measurements. Diurnal variations of the radon concentration in air at ground level also occur because of different varying turbulent mixing: the concentrations are maximum in the early morning and minimum in the afternoon. The variations are generally less than one order of magnitude.
[WHO; Environ Health Criteria: Selected Radionuclides (radon) p.151 (1983)]**PEER REVIEWED**
In the composition of dry air, nine principal constituents are constant wherever free air is sampled. Five of these are the stable helium-group gases. Other trace impurities in air vary in concentration from place to place; among these is radon. The longest lived isotope, 222Rn, has a half-life of 3.825 days which is short compared to the atmosphere's mixing time.
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 6]**PEER REVIEWED**
Radon gaseous concn in air (vol %): 6X10-18% (20 km altitude) (gas)
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V17 (95) 924]**PEER REVIEWED**
Other Environmental Concentrations:
Radon in houses comes from building materials, the soil under the house, the water, and the domestic gas. Radium concentrations in building materials have been investigated. The data indicate the some materials such as aerated concrete with alum shale and phospho-gypsum from sedimentary ores have significantly higher radium concentrations than others and cause enhanced radon concentrations indoors. If these materials are excluded, the average concentrations of radium in building material is about 100 becquerel/kg. Materials with low activity are wood, natural gypsum, sand, and gravel. The radon exhalation rate from walls, floors, and ceilings is dependent on the radium concentration, the emanation power, the diffusion coefficient in the material and the qualities and thickness of any applied sealant on the surfaces.
[WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.145-6 (1983)]**PEER REVIEWED**
In view of the strong influence of the ventilation rate, there are great variations of the radon levels as the effective ventilation of a room is changed. This is caused by meteorological conditions (wind, pressure, temperature) and by human activities like opening doors and windows. There may be variations of the radon concentration in air caused by changes of the radon exhalation rate from surfaces, which in turn can be caused by changes of atmospheric pressure.
[Johassen N; Health Phys 29: 216-20 (1975) as cited in WHO; Environ Health Criteria: Selected Radionuclides (Radon) p.153 (1983)]**PEER REVIEWED**
Environmental Standards & Regulations:
CERCLA Reportable Quantities:
Persons in charge of vessels or facilities are required to notify the National Response Center (NRC) immediately, when there is a release of this designated hazardous substance, in an amount equal to or greater than its reportable quantity of 0.1 curie or 3.7x10+9 becquerel. The toll free number of the NRC is (800) 424-8802; In the Washington D.C. metropolitan area (202) 426-2675. The rule for determining when notification is required is stated in 40 CFR 302.4 (section IV. D.3.b). /(220)Radon/
[40 CFR 302.4 (7/1/99)]**PEER REVIEWED**
Persons in charge of vessels or facilities are required to notify the National Response Center (NRC) immediately, when there is a release of this designated hazardous substance, in an amount equal to or greater than its reportable quantity of 0.1 curie or 3.7x10+9 becquerel. The toll free number of the NRC is (800) 424-8802; In the Washington D.C. metropolitan area (202) 426-2675. The rule for determining when notification is required is stated in 40 CFR 302.4 (section IV. D.3.b). /(222)Radon/
[40 CFR 302.4 (7/1/99)]**PEER REVIEWED**
Atmospheric Standards:
Radionuclides have been designated as a hazardous air pollutant under section 112 of the Clean Air Act. /Radionuclides/
[40 CFR 61.01 (7/1/99)]**PEER REVIEWED**
Listed as a hazardous air pollutant (HAP) generally known or suspected to cause serious health problems. The Clean Air Act, as amended in 1990, directs EPA to set standards requiring major sources to sharply reduce routine emissions of toxic pollutants. EPA is required to establish and phase in specific performance based standards for all air emission sources that emit one or more of the listed pollutants. Radon is included on this list.
[Clean Air Act as amended in 1990, Sect. 112 (b) (1) Public Law 101-549 Nov. 15, 1990]**PEER REVIEWED**
State Drinking Water Guidelines:
(MA) MASSACHUSETTS 10000 pCi/l
[USEPA/Office of Water; Federal-State Toxicology and Risk Analysis Committee (FSTRAC). Summary of State and Federal Drinking Water Standards and Guidelines (11/93), p. ]**QC REVIEWED**
Chemical/Physical Properties:
Molecular Formula:
Rn
[Sax, N.I. and R.J. Lewis, Sr. (eds.). Hawley's Condensed Chemical Dictionary. 11th ed. New York: Van Nostrand Reinhold Co., 1987., p. 995]**PEER REVIEWED**
Molecular Weight:
222
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-79]**PEER REVIEWED**
Color/Form:
Colorless gas
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
Can be condensed to a colorless, transparent liquid & to an opaque, glowing solid.
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
When cooled below the freezing point, radon exhibits a brilliant phosphorescence which becomes yellow as the temperature is lowered and orange-red at the temperature of liquid air.
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-24]**PEER REVIEWED**
Solid form exists as face-centered cubic crystals at normal pressure.
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Odor:
Odorless
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Taste:
Tasteless
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Boiling Point:
-61.7 deg C (liquid)
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-79]**PEER REVIEWED**
Melting Point:
-71 deg C
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 4-79]**PEER REVIEWED**
Critical Temperature & Pressure:
Critical temperature: 104 deg C; Critical pressure: 6.28 MPa
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 6-48]**PEER REVIEWED**
Density/Specific Gravity:
9.72 g/l, (0 deg C)
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
Heat of Vaporization:
18,000 J/mol (normal bp)
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Solubilities:
In water, 230 ml/kg @ 20 deg C
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 6]**PEER REVIEWED**
51.0 cu cm/100 cc of water @ 0 deg C
[Weast, R.C. (ed.) Handbook of Chemistry and Physics. 69th ed. Boca Raton, FL: CRC Press Inc., 1988-1989., p. B-122]**PEER REVIEWED**
22.4 cu cm/100 cc of water @ 25 deg C
[Weast, R.C. (ed.) Handbook of Chemistry and Physics. 69th ed. Boca Raton, FL: CRC Press Inc., 1988-1989., p. B-122]**PEER REVIEWED**
Slightly soluble in alcohol & organic liquids
[Weast, R.C. (ed.) Handbook of Chemistry and Physics. 69th ed. Boca Raton, FL: CRC Press Inc., 1988-1989., p. B-122]**PEER REVIEWED**
0.326 ml/1 ml water @ 10 deg C
[Dean, J.A. Handbook of Organic Chemistry. New York, NY: McGraw-Hill Book Co., 1987., p. 4-7]**PEER REVIEWED**
0.222 ml/1 ml water @ 20 deg C
[Dean, J.A. Handbook of Organic Chemistry. New York, NY: McGraw-Hill Book Co., 1987., p. 4-7]**PEER REVIEWED**
0.162 ml/1 ml water @ 30 deg C
[Dean, J.A. Handbook of Organic Chemistry. New York, NY: McGraw-Hill Book Co., 1987., p. 4-7]**PEER REVIEWED**
0.126 ml/1 ml water @ 40 deg C
[Dean, J.A. Handbook of Organic Chemistry. New York, NY: McGraw-Hill Book Co., 1987., p. 4-7]**PEER REVIEWED**
0.085 ml/1 ml water @ 60 deg C
[Dean, J.A. Handbook of Organic Chemistry. New York, NY: McGraw-Hill Book Co., 1987., p. 4-7]**PEER REVIEWED**
13.0 cu m/100 cu m water @ 50 deg C
[IARC. Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Man. Geneva: World Health Organization, International Agency for Research on Cancer, 1972-PRESENT. (Multivolume work)., p. V43 173 (1988)]**PEER REVIEWED**
Spectral Properties:
Characteristic Emission Lines: K(alpha2)KL2= 0.15294; K(beta3)KM2= 0.13155; L(alph2)L3M4= 1.06899.
[Robinson JW (ed.); Handbook of Spectroscopy Vol 1 Baton Rouge, La: CRC Press Inc., 20 (1979)]**PEER REVIEWED**
Vapor Pressure:
1 Pa @ -163 deg C; 10 Pa @ -152 deg C; 100 Pa @ -139 deg C; 1 kPa @ -121.4 deg C; 10 kPa @ -97.6 deg C (solid)
[Lide, D.R. (ed.). CRC Handbook of Chemistry and Physics. 79th ed. Boca Raton, FL: CRC Press Inc., 1998-1999., p. 6-65]**PEER REVIEWED**
Viscosity:
23.3 Pa.s @ 101.32 kPa, 25 deg C (gas)
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 6]**PEER REVIEWED**
Other Chemical/Physical Properties:
18 radioactive isotopes, all short lived
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
The heaviest gas known.
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
Heat of fusion: 3247 J/mol
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 6]**PEER REVIEWED**
The half-life of (220)radon is 55.6 seconds. /(220)Radon/
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
The half-life of (222)radon is 3.825 days. /(222)Radon/
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
The half-life of (219)radon is 3.96 seconds. /(219)Radon/
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Chemical Safety & Handling:
Hazardous Reactivities & Incompatibilities:
It has been reported that fluorine reacts with radon, forming radon fluoride.
[Weast, R.C. (ed.) Handbook of Chemistry and Physics. 69th ed. Boca Raton, FL: CRC Press Inc., 1988-1989., p. B-31]**PEER REVIEWED**
Protective Equipment & Clothing:
Respiratory protection shall be used by miners when work practices and engineering controls are not adequate to limit average work shift concentration of radon progeny to 1/12 the average work shift concentration, when entering a mine area where concentrations of radon progeny are unknown or during emergencies. Use only those respirators /SRP: certified/ by NIOSH or the Mine Safety and Health Administration.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.8 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
The mine operator shall provide facilities so that miners can wash their hands and faces thoroughly with soap or mild detergent and water before eating or drinking ... provide an adequate number of toilet facilities and encourage the miners to wash their hands thoroughly with soap or mild detergent and water before and after using these facilities ... provide clean change rooms ... storage facilities such as lockers to permit the miners to store street clothing and personal items. The mine operator shall provide showers and encourage the miners to shower at the end of the work shift ... cleaning, laundering, or disposal of contaminated work clothing or equipment. Any person who cleans or launders this contaminated work clothing or equipment must be informed by the operator that it may be contaminated with radioactive materials.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p. 13 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": ... dispensers of liq detergent /should be available/. ... Safety pipettes should be used for all pipetting. ... In animal laboratory, personnel should ... wear protective suits (preferably disposable, one-piece & close-fitting at ankles & wrists), gloves, hair covering & overshoes. ... In chemical laboratory, gloves & gowns should always be worn ... however, gloves should not be assumed to provide full protection. Carefully fitted masks or respirators may be necessary when working with particulates or gases, & disposable plastic aprons might provide addnl protection. ... gowns ... /should be/ of distinctive color, this is a reminder that they are not to be worn outside the laboratory. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 8]**PEER REVIEWED**
Preventive Measures:
... Measures that can be taken to reduce exposure to radon are described, including replacement of fill, surface coating of building foundations, air filtration and improved ventilation. ...
[Tartaglia M et al; J Environ Health 47 (2): 62-7 (1986)]**PEER REVIEWED**
There are three general categories of techniques for the control of radon and radon progeny concentrations in indoor air: restriction of radon entry, reduction of indoor radon concentrations by ventilation or air cleaning, and removal of airborne radon progeny. The predominant radon entry process in most residences appears to be pressure driven flow of soil gas through cracks or other openings in the basement, slab or subfloor. Sealing these openings or ventilation of the subslab or subfloor space are methods of reducing radon entry rates. Indoor radon concentrations may be reduced by increased ventilation. The use of charcoal filters for removal of radon gas in the indoor air by adsorption has also been proposed. Concentrations of radon associated with radon exposures, can be controlled by use of electrostatic or mechanical filtration. Air circulation can also reduce radon progeny concentrations in certain cases. ... Reviews of the application and limitations of each of these control measures /are also discussed/.
[Sextra RG; Govt Reports Announcements & Index (5): (1986)]**PEER REVIEWED**
Effective work practices and engineering controls shall be instituted by the mine operator to reduce the concentration of radon progeny to the lowest technically achievable limit. ... 1. Ore extraction and Handling: Examples of effective ore extraction and handling procedures include the following: minimizing the number of ore faces simultaneously exposed, performing retreat mining toward intake air, limiting the underground storage and handling of ore, locating ore transfer points away from ventilation intakes, removing dust spilled from ore cars, minimizing ore spillage by maintaining roadways and carefully loading haulage vehicles and covering ore until it is moved to the surface. 2. Blasting should be performed at the end of the work shift whenever possible. Miners shall be evacuated from exhaust drifts until environmental sampling confirms that the average work shift concentration of radon progeny does not exceed 1/12 of a working level concentration. The mine operator shall not use the planned rotation of miners to maintain an individual's exposure below the recommended exposure limit of 1.0 working level month per year.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.6 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
Mechanical exhaust ventilation used alone or in combination with other engineering controls and work practices can effectively reduce exposures to radon progeny. Ventilation systems discharging outside the mine shall conform with applicable local, state, and federal air pollution regulations and shall not constitute a hazard to miners or to the general population. ... Fans shall be operated continuously in the work areas of an active mine and before the opening of a previously inactive mine or inactive section until environmental sampling confirms that the average work shift concentrations of radon progeny do not exceed 1/12 an average work shift concentration.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.7 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
The preparation, storage, dispensing (including vending machines), or consumption of food shall be prohibited in any area where a toxic material is present.
[NIOSH; Criteria for a Recommended Standard, Occupational Exposure to Radon Progeny in Underground Mines p.13 (1987) DHHS Pub. NIOSH 88-101]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Smoking, drinking, eating, storage of food or of food & beverage containers or utensils, & the application of cosmetics should be prohibited in any laboratory. All personnel should remove gloves, if worn, after completion of procedures in which carcinogens have been used. They should ... wash ... hands, preferably using dispensers of liq detergent, & rinse ... thoroughly. Consideration should be given to appropriate methods for cleaning the skin, depending on nature of the contaminant. No standard procedure can be recommended, but the use of organic solvents should be avoided. Safety pipettes should be used for all pipetting. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 8]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": In animal laboratory, personnel should remove their outdoor clothes & wear protective suits (preferably disposable, one-piece & close-fitting at ankles & wrists), gloves, hair covering, & overshoes. ... clothing should be changed daily but ... discarded immediately if obvious contamination occurs ... /also,/ workers should shower immediately. In chemical laboratory, gloves & gowns should always be worn ... however, gloves should not be assumed to provide full protection. Carefully fitted masks or respirators may be necessary when working with particulates or gases, & disposable plastic aprons might provide addnl protection. If gowns are of distinctive color, this is a reminder that they should not be worn outside of lab. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 8]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": ... operations connected with synth & purification ... should be carried out under well-ventilated hood. Analytical procedures ... should be carried out with care & vapors evolved during ... procedures should be removed. ... Expert advice should be obtained before existing fume cupboards are used ... & when new fume cupboards are installed. ... Glove boxes should be kept under negative air pressure. Air changes should be adequate, so that concn of vapors of volatile carcinogens will not occur. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 8]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Vertical laminar-flow biological safety cabinets may be used for containment of in vitro procedures ... provided that the exhaust air flow is sufficient to provide an inward air flow at the face opening of the cabinet, & contaminated air plenums that are under positive pressure are leak-tight. Horizontal laminar-flow hoods or safety cabinets, where filtered air is blown across the working area towards the operator, should never be used. ... Each cabinet or fume cupboard to be used ... should be tested before work is begun (eg, with fume bomb) & label fixed to it, giving date of test & avg air-flow measured. This test should be repeated periodically & after any structural changes. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 9]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Principles that apply to chem or biochem lab also apply to microbiological & cell-culture labs. ... Special consideration should be given to route of admin. ... Safest method of administering volatile carcinogen is by injection of a soln. Admin by topical application, gavage, or intratracheal instillation should be performed under hood. If chem will be exhaled, animals should be kept under hood during this period. Inhalation exposure requires special equipment. ... unless specifically required, routes of admin other than in the diet should be used. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 9]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": To eliminate risk that ... contamination in lab could build up during conduct of expt, periodic checks should be carried out on lab atmospheres, surfaces, such as walls, floors & benches, & ... interior of fume hoods & air ducts. As well as regular monitoring, check must be carried out after cleaning-up of spillage. Sensitive methods are required when testing lab atmospheres. ... Methods ... should ... where possible, be simple & sensitive. ... /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 10]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Rooms in which obvious contamination has occurred, such as spillage, should be decontaminated by lab personnel engaged in expt. Design of expt should ... avoid contamination of permanent equipment. ... Procedures should ensure that maintenance workers are not exposed to carcinogens. ... Particular care should be taken to avoid contamination of drains or ventilation ducts. In cleaning labs, procedures should be used which do not produce aerosols or dispersal of dust, ie, wet mop or vacuum cleaner equipped with high-efficiency particulate filter on exhaust, which are avail commercially, should be used. Sweeping, brushing & use of dry dusters or mops should be prohibited. Grossly contaminated cleaning materials should not be re-used ... If gowns or towels are contaminated, they should not be sent to laundry, but ... decontaminated or burnt, to avoid any hazard to laundry personnel. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 10]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Doors leading into areas where carcinogens are used ... should be marked distinctively with appropriate labels. Access ... limited to persons involved in expt. ... A prominently displayed notice should give the name of the Scientific Investigator or other person who can advise in an emergency & who can inform others (such as firemen) on the handling of carcinogenic substances. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 11]**PEER REVIEWED**
SRP: Contaminated protective clothing should be segregated in such a manner so that there is no direct personal contact by personnel who handle, dispose, or clean the clothing. Quality assurance to ascertain the completeness of the cleaning procedures should be implemented before the decontaminated protective clothing is returned for reuse by the workers. Contaminated clothing should not be taken home at end of shift, but should remain at employee's place of work for cleaning.
**PEER REVIEWED**
Control of radon and its daughters is accomplished generally by ventilation.
[Zenz, C., O.B. Dickerson, E.P. Horvath. Occupational Medicine. 3rd ed. St. Louis, MO., 1994, p. 414]**PEER REVIEWED**
Shipment Methods and Regulations:
PRECAUTIONS FOR "CARCINOGENS": Procurement ... of unduly large amt ... should be avoided. To avoid spilling, carcinogens should be transported in securely sealed glass bottles or ampoules, which should themselves be placed inside strong screw-cap or snap-top container that will not open when dropped & will resist attack from the carcinogen. Both bottle & the outside container should be appropriately labelled. ... National post offices, railway companies, road haulage companies & airlines have regulations governing transport of hazardous materials. These authorities should be consulted before ... material is shipped. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 13]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": When no regulations exist, the following procedure must be adopted. The carcinogen should be enclosed in a securely sealed, watertight container (primary container), which should be enclosed in a second, unbreakable, leakproof container that will withstand chem attack from the carcinogen (secondary container). The space between primary & secondary container should be filled with absorbent material, which would withstand chem attack from the carcinogen & is sufficient to absorb the entire contents of the primary container in the event of breakage or leakage. Each secondary container should then be enclosed in a strong outer box. The space between the secondary container & the outer box should be filled with an appropriate quantity of shock-absorbent material. Sender should use fastest & most secure form of transport & notify recipient of its departure. If parcel is not received when expected, carrier should be informed so that immediate effort can be made to find it. Traffic schedules should be consulted to avoid ... arrival on weekend or holiday ... /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 13]**PEER REVIEWED**
Storage Conditions:
Radon and its daughters build up to an equilibrium value in about a month from radium cmpd ... good ventilation of areas where radium is handled or stored is recommended to prevent accumulations of hazardous concentrations of radon and its daughters.
[Sax, N.I. Dangerous Properties of Industrial Materials. 6th ed. New York, NY: Van Nostrand Reinhold, 1984., p. 2357]**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": Storage site should be as close as practicable to lab in which carcinogens are to be used, so that only small quantities required for ... expt need to be carried. Carcinogens should be kept in only one section of cupboard, an explosion-proof refrigerator or freezer (depending on chemicophysical properties ...) that bears appropriate label. An inventory ... should be kept, showing quantity of carcinogen & date it was acquired ... Facilities for dispensing ... should be contiguous to storage area. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 13]**PEER REVIEWED**
Cleanup Methods:
PRECAUTIONS FOR "CARCINOGENS": A high-efficiency particulate arrestor (HEPA) or charcoal filters can be used to minimize amt of carcinogen in exhausted air, ventilated safety cabinets, lab hoods, glove boxes or animal rooms ... Filter housing that is designed so that used filters can be transferred into plastic bags without contaminating maintenance staff is avail commercially. Filters should be placed in plastic bags immediately after removal ... The plastic bag should be sealed immediately ... The sealed bag should be labelled properly ... Waste liquids ... should be placed or collected in proper containers for disposal. The lid should be secured & the bottles properly labelled. Once filled, bottles should be placed in plastic bag, so that outer surface ... is not contaminated ... The plastic bag should also be sealed & labelled. ... Broken glassware ... should be decontaminated by solvent extraction, by chemical destruction, or in specially designed incinerators. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 15]**PEER REVIEWED**
Disposal Methods:
SRP: At the time of review, criteria for land treatment or burial (sanitary landfill) disposal practices are subject to significant revision. Prior to implementing land disposal of waste residue (including waste sludge), consult with environmental regulatory agencies for guidance on acceptable disposal practices.
**PEER REVIEWED**
PRECAUTIONS FOR "CARCINOGENS": There is no universal method of disposal that has been proved satisfactory for all carcinogenic compounds & specific methods of chem destruction ... published have not been tested on all kinds of carcinogen-containing waste. ... summary of avail methods & recommendations ... /given/ must be treated as guide only. /Chemical Carcinogens/
[Montesano, R., H. Bartsch, E.Boyland, G. Della Porta, L. Fishbein, R. A. Griesemer, A.B. Swan, L. Tomatis, and W. Davis (eds.). Handling Chemical Carcinogens in the Laboratory: Problems of Safety. IARC Scientific Publications No. 33. Lyon, France: International Agency for Research on Cancer, 1979., p. 14]**PEER REVIEWED**
Occupational Exposure Standards:
Manufacturing/Use Information:
Major Uses:
Medicine (cancer treatment)/former use/, tracer in leak detection, flow-rate measurement, radiography, chemical research.
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
There are no significant technical uses for radon.
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 25]**PEER REVIEWED**
To initiate and influence chemical reactions, as a surface label in the study of surface reactions; in the determination of radium or thorium; in the study of the behavior of filters; in combination with Be or other light materials as a source of neutrons.
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Therap cat: Antineoplastic (radiation source)
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Methods of Manufacturing:
Derived from the radioactive decay of radium. Radon is obtained by bubbling air through a radon salt solution and collecting the gas plus air.
[Lewis, R.J., Sr (Ed.). Hawley's Condensed Chemical Dictionary. 13th ed. New York, NY: John Wiley & Sons, Inc. 1997., p. 955]**PEER REVIEWED**
The various isotopes of radon, all having short half-lives, are formed by the radioactive decay of radium, actinium, and thorium.
[Kirk-Othmer Encyclopedia of Chemical Technology. 4th ed. Volumes 1: New York, NY. John Wiley and Sons, 1991-Present., p. V13 (95) 3]**PEER REVIEWED**
General Manufacturing Information:
A working level month is defined as a 170 hr working month exposure to alpha radiation from radon daughters equal to 1.3X10+5 megaelectron volts emitted in 1 liter of air.
[Harely N et al; Environmental Health Perspectives 70: 17-21 (1986)]**PEER REVIEWED**
1 g of radium produces about 0.0001 ml of radon/day @ normal temp and pressure /Radium/
[Budavari, S. (ed.). The Merck Index - An Encyclopedia of Chemicals, Drugs, and Biologicals. Whitehouse Station, NJ: Merck and Co., Inc., 1996., p. 1393]**PEER REVIEWED**
Laboratory Methods:
Analytic Laboratory Methods:
Definitions and units appropriate for radon and radon daughters are given. The principle methods of detection are ionization chamber, scintillation technique, nuclear track detector, thermoluminescent discs, and alpha spectrometry. The activity concentration is determined by grab sampling and subsequent measurement, frequent or continuous grab sampling and measurement and continuous sampling and long time integrated measurement. Sampling and measurement strategies for mines, dwellings, and the environment are discussed.
[Snihs JD; Govt Reports Announcements & Index 9: (1985)]**PEER REVIEWED**
Special References:
Special Reports:
Borak TB, Johnson JA; Estimating the Risk of Lung Cancer from Inhalation of Radon Daughters Indoors: Review and Evaluaton, Gov't Reports Announcements and Index 18: 1-131 (1988).
Doege TC, Hendee WR; Semin Nucl Med 18 (1): 10-15 (1988)
Fish WJ; Research Review: Indoor Air Quality Control Techniques, Gov't Reports Announcements and Index 19: 1-37 (1987)
Ernst P, Theriault G; Can Med Assoc J 130 (7): 863-7 (1984)
USEPA; Drinking Water Criteria Document for Radon (Draft) (1986)
USEPA; Review of the Office of Radiation Programs National Radon Survey Design Gov't Reports Announcements and Index 24: 1-18 (1988)
Anon; Scientific Basis for Risk Assessment and Management of Uranium Mill Tailings, Gov't Reports Announcements and Index 11: 1-262 (1988)
Becker AP III, Lachajozyk TM; Evaluation of Waterborne Radon Impact on Indoor Air Quality and Assessment of Control Options, Gov't Reports Announcements and Index 25: 1-146 (1984)
DHHS/ATSDR; Toxicological Profile for Radon (1990) ATSDR/TP-90/23
U.S. Department of Health & Human Services/National Toxicology Program; Tenth Report on Carcinogens. National Institutes of Environmental Health Sciences. The Report on Carcinogens is an informational scientific and public health document that identifies and discusses substances (including agents, mixtures, or exposure circumstances) that may pose a carcinogenic hazard to human health. ( Radon (10043-92-7) was first listed in the Seventh Annual Report on Carcinogens (1994) as known to be a human carcinogen.
[ ]
Synonyms and Identifiers:
Related HSDB Records:
2146 [RADIUM]
Synonyms:
Alphatron
**PEER REVIEWED**
Niton /(222)Radon/
**PEER REVIEWED**
Radium emanation
**PEER REVIEWED**
Associated Chemicals:
RADON-222;14859-67-7
POLONIUM-218;15422-74-9
POLONIUM-214;15735-67-8
POLONIUM-210;13981-52-7
POLONIUM-216;15756-58-8
POLONIUM-215;15706-52-2
Test Your Home for this Radioactive Gas